Understanding the DWC PR-3 form is crucial for anyone navigating the complexities of workers' compensation claims in California. Designed for use by a primary treating physician, this form plays a pivotal role in the evaluation and reporting of an individual's permanent disability post-injury. Essentially, it provides a comprehensive overview of the patient's condition once it has stabilized to a point known as permanent and stationary, indicating that the patient has reached maximum medical improvement. This form covers a broad spectrum of information including diagnostic tests, medical history, objective and subjective findings, and recommendations for future medical care if necessary. It's important to note that the DWC PR-3 is not intended for use by Qualified Medical Evaluators (QME) or Agreed Medical Evaluators (AME) in their medical-legal evaluations but is instead specifically designed for the primary treating physician to communicate the patient's condition, limitations, and further treatment needs directly to the claims administrator. This process ensures that the patient's care and any compensation claims are handled accurately based on a thorough medical assessment.
| Question | Answer |
|---|---|
| Form Name | Dwc Form Pr 3 |
| Form Length | 5 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min 15 sec |
| Other names | pr3 physicians evaluation of permanent and stationary state of ca form |
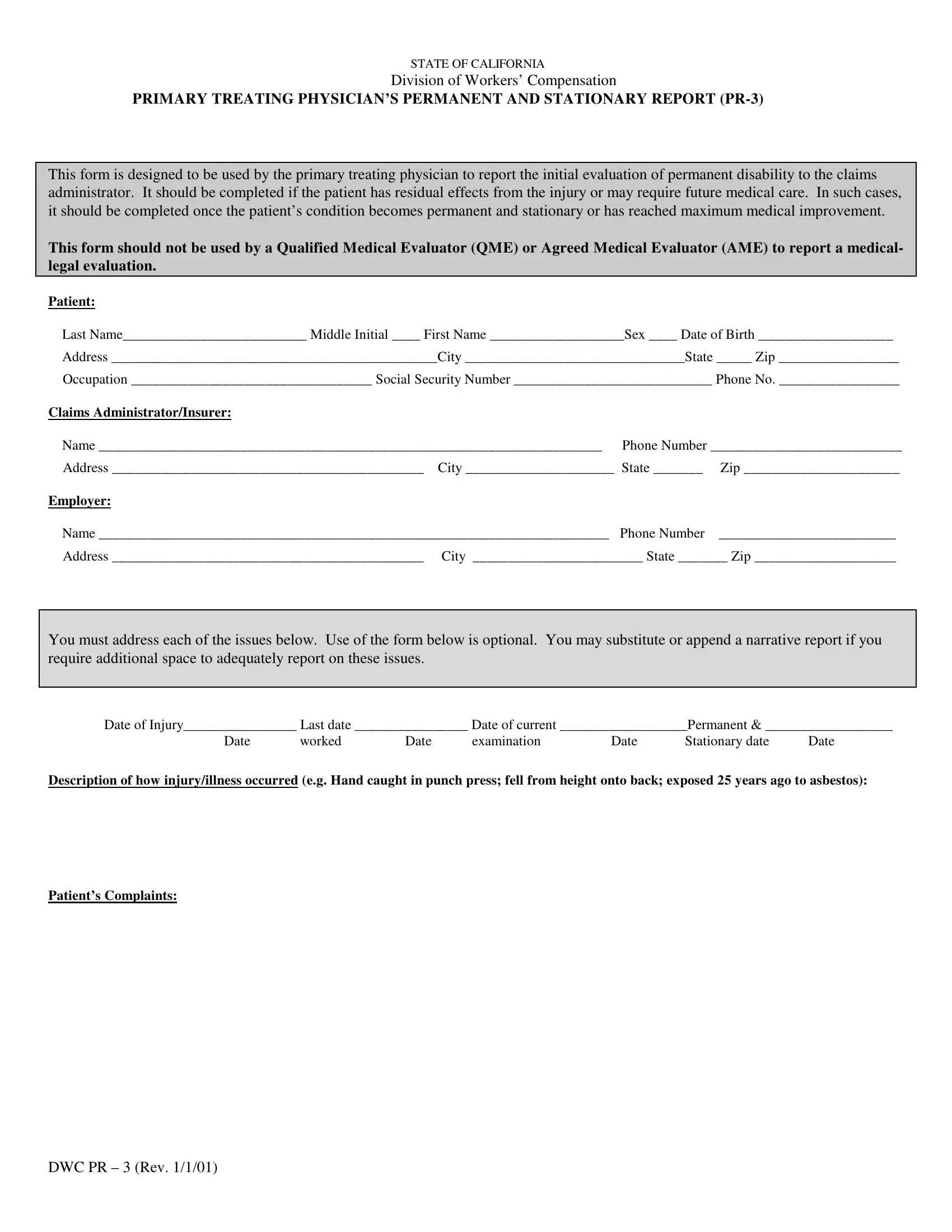
STATE OF CALIFORNIA
Division of Workers’ Compensation
PRIMARY TREATING PHYSICIAN’S PERMANENT AND STATIONARY REPORT
This form is designed to be used by the primary treating physician to report the initial evaluation of permanent disability to the claims administrator. It should be completed if the patient has residual effects from the injury or may require future medical care. In such cases, it should be completed once the patient’s condition becomes permanent and stationary or has reached maximum medical improvement.
This form should not be used by a Qualified Medical Evaluator (QME) or Agreed Medical Evaluator (AME) to report a medical- legal evaluation.
Patient:
Last Name__________________________ Middle Initial ____ First Name ___________________Sex ____ Date of Birth ___________________
Address ______________________________________________City _______________________________State _____ Zip _________________
Occupation __________________________________ Social Security Number ____________________________ Phone No. _________________
Claims Administrator/Insurer: |
|
|
|
Name _______________________________________________________________________ |
Phone Number ___________________________ |
||
Address ____________________________________________ |
City _____________________ State _______ |
Zip ______________________ |
|
Employer: |
|
|
|
Name ________________________________________________________________________ |
Phone Number |
_________________________ |
|
Address ____________________________________________ |
City ________________________ State _______ Zip ____________________ |
||
You must address each of the issues below. Use of the form below is optional. You may substitute or append a narrative report if you require additional space to adequately report on these issues.
Date of Injury________________ Last date ________________ Date of current __________________Permanent & __________________
Date |
worked |
Date |
examination |
Date |
Stationary date |
Date |
Description of how injury/illness occurred (e.g. Hand caught in punch press; fell from height onto back; exposed 25 years ago to asbestos):
Patient’s Complaints:
DWC PR – 3 (Rev. 1/1/01)

STATE OF CALIFORNIA
Division of Workers’ Compensation
PRIMARY TREATING PHYSICIAN’S PERMANENT AND STATIONARY REPORT
Relevant Medical History:
Objective Findings:
Physical Examination: (Describe all relevant findings; include any specific measurements indicating atrophy, range of motion, strength, etc.; include bilateral measurements - injured/uninjured - for upper and lower extremity injuries.)
Diagnostic tests results
Diagnoses (List each diagnosis; |
||
1. |
|
______________________________________ |
2. |
|
______________________________________ |
3. |
__________________________________________________________________ |
______________________________________ |
4. |
__________________________________________________________________ |
______________________________________ |
|
Yes |
No |
Cannot determine |
Did work cause or contribute to the injury or illness? |
V |
V |
V |
Apportionment:
Are there
any documentation of
Can this patient now return to his/her usual occupation? |
V |
V |
V |
If not, can the patient perform another line of work? |
V |
V |
V |
DWC Form
2

STATE OF CALIFORNIA
Division of Workers’ Compensation
PRIMARY TREATING PHYSICIAN’S PERMANENT AND STATIONARY REPORT
Subjective Findings: Provide your professional assessment of the subjective factors of disability, based on your evaluation of the patient’s complaints, your examination, and other findings. List specific symptoms (e.g. pain right wrist) and their frequency, severity, and/or precipitating activity using the following definitions:
Severity: Minimal pain (Min) - an annoyance, causes no handicap in performance. Slight pain (Slt) - tolerable, causes some handicap in performance of the activity precipitating pain. Moderate pain (Mod) - tolerable, causes marked handicap in the performance of the activity precipitating pain. Severe pain (Sev) - precludes performance of the activity precipitating pain.
Frequency: Occasional (Occ) - occurs roughly one fourth of the time. Intermittent (Int) - occurs roughly one half of the time. Frequent (Fre) - occurs roughly three fourths of the time. Constant (Con) - occurs roughly 90 to 100% of time.
Precipitating activity: Precipitating activity gives a sense of how often a pain is felt and thus is often provided in lieu of frequency, e.g. slight pain in back on heavy lifting, or
Symptom |
|
Frequency |
|
|
Severity |
|
|
|
|
Precipitating |
|||||
|
(Mark X at any spot) |
(Mark X at any spot.) |
Activity |
||||||||||||
| |
| |
|
|||||||||||||
|
Occ |
|
Int |
|
Fre |
|
Con |
Min |
|
Slt |
|
Mod |
Sev |
|
|
| |
| |
|
|||||||||||||
|
Occ |
|
Int |
|
Fre |
|
Con |
Min |
|
Slt |
|
Mod |
|
Sev |
|
| |
| |
|
|||||||||||||
|
Occ |
|
Int |
|
Fre |
|
Con |
Min |
|
Slt |
|
Mod |
|
Sev |
|
| |
| |
|
|||||||||||||
|
Occ |
|
Int |
|
Fre |
|
Con |
Min |
|
Slt |
|
Mod |
|
Sev |
|
|
Yes |
No |
Cannot determine |
V |
V |
V |
|
as well now as could be done prior to this injury or illness? |
|
|
|
If yes, please describe
1.
2.
3.
4.
DWC Form
3
STATE OF CALIFORNIA
Division of Workers’ Compensation
PRIMARY TREATING PHYSICIAN’S PERMANENT AND STATIONARY REPORT
Preclusions/Work Restrictions |
|
|
|
|
Yes |
No |
Cannot determine |
Are there any activities the patient cannot do? |
V |
V |
V |
If yes, please describe all preclusions or restrictions related to work activities (e.g. no lifting more than 10 lbs. above shoulders; must use splint; keyboard only 45 mins. per hour; must have sit/stand workstation; no repeated bending). Include restrictions which may not be relevant to current job but may affect future efforts to find work on the open labor market (e.g. include lifting restriction even if current job requires no lifting; include limits on repetitive hand movements even if current job requires none).
1.
2.
3.
4.
5.
6.
Future Medical Treatment: Describe any medical treatment related to this injury that you believe the patient may require in the future. Include medications, surgery, physical medicine services, durable equipment, etc.
Comments:
DWC Form
4

STATE OF CALIFORNIA
Division of Workers’ Compensation
PRIMARY TREATING PHYSICIAN’S PERMANENT AND STATIONARY REPORT
List any other physicians who contributed information used in this report: |
|
|
|
A. |
Name ______________________________________________ |
Specialty ________________________________________________ |
|
B. |
Name ______________________________________________ |
Specialty ________________________________________________ |
|
C. |
Name ______________________________________________ |
Specialty ________________________________________________ |
|
List information you reviewed in preparing this report, or relied upon for the formulation of your medical opinions: |
|||
Medical Records |
Personnel Records |
||
Written Job Description |
Any other, please describe: |
Primary Treating Physician (original signature, do not stamp)
I declare under penalty of perjury that this report is true and correct to the best of my knowledge, and that I have not violated Labor Code §139.3.
Signature : |
|
|
|
|
Cal. Lic. # : __________________________ _ |
|||
|
|
|
|
|
|
|
|
|
Executed at : |
|
|
|
|
Date: __________________________________ |
|||
|
|
(County and State) |
|
|
|
|
|
|
Name (Printed) : |
|
|
|
|
Specialty: _______________________________ |
|||
Address : _________________________________________ |
City: ___________________ State: __________Zip : _________ |
|||||||
Telephone: ______________________________________ |
|
|
|
|
|
|
||
DWC Form
5