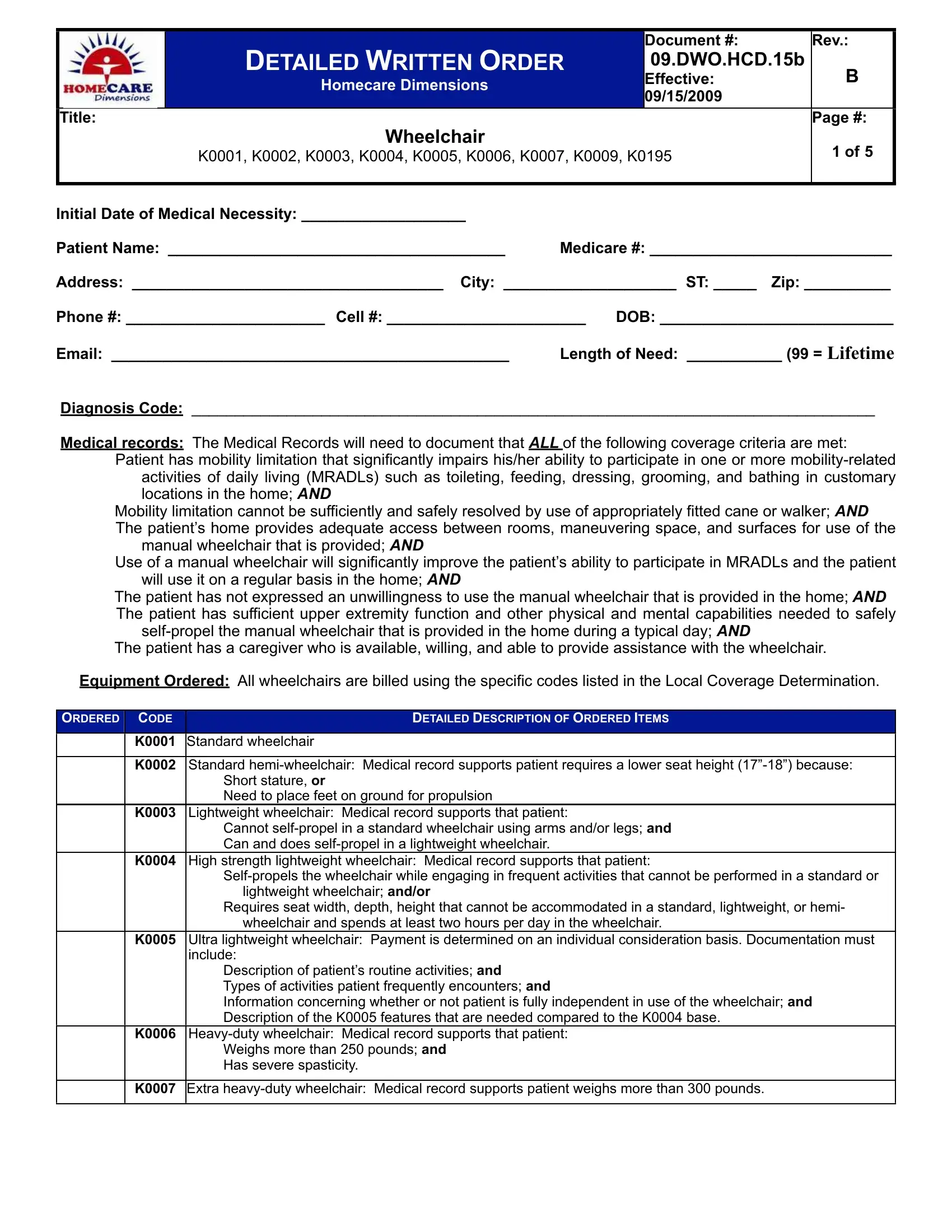
The Detailed Written Order (DWO) form, specifically referenced as 09.DWO.HCD.15b for Homecare Dimensions, effective from September 15, 2009, stands as a comprehensive document designed to ensure the appropriate and necessary provision of wheelchairs to patients. This form encompasses various aspects, including but not limited to, the initial date of medical necessity, patient's identification and contact information, diagnosis code, and a thorough listing of medical records that substantiate the coverage criteria for the mobility aid. Crucially, it outlines the conditions under which a patient is considered eligible for a wheelchair, emphasizing the inability to perform mobility-related activities of daily living (MRADLs) with canes or walkers, the home environment's suitability for wheelchair maneuvering, and the regular use and physical capability to operate the provided wheelchair. The form meticulously details the types and specifications of ordered wheelchairs – from standard to ultra-lightweight and heavy-duty models – based on the patient’s specific medical needs and daily activities. Furthermore, it integrates a system of checks for both the ordering physician and the patient, through signatures and attestations, to confirm the necessity and agreement toward the prescribed mobility solution. This document not only facilitates a structured approach to assessing and documenting patient needs but also serves as a critical tool in aligning medical provisions with payer coverage policies, thereby ensuring that patients receive the essential support for their mobility challenges.
| Question | Answer |
|---|---|
| Form Name | Dwo Form |
| Form Length | 5 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min 15 sec |
| Other names | dwo medicare form pdf, detailed written order template, medicare dwo, behavior forms pdf |
