



Once you open the online editor for PDFs by FormsPal, you can fill out or modify emedny form 436601 here and now. Our tool is continually evolving to grant the very best user experience possible, and that's because of our dedication to continual enhancement and listening closely to user opinions. To get the process started, take these simple steps:
Step 1: Press the orange "Get Form" button above. It's going to open our pdf editor so that you can start completing your form.
Step 2: Using this advanced PDF editing tool, you're able to accomplish more than simply fill in forms. Express yourself and make your documents look perfect with customized text added, or optimize the file's original input to perfection - all comes with an ability to add almost any graphics and sign the PDF off.
Be mindful when filling in this pdf. Make sure each field is filled out correctly.
1. Start completing the emedny form 436601 with a number of necessary fields. Collect all of the information you need and make sure absolutely nothing is left out!
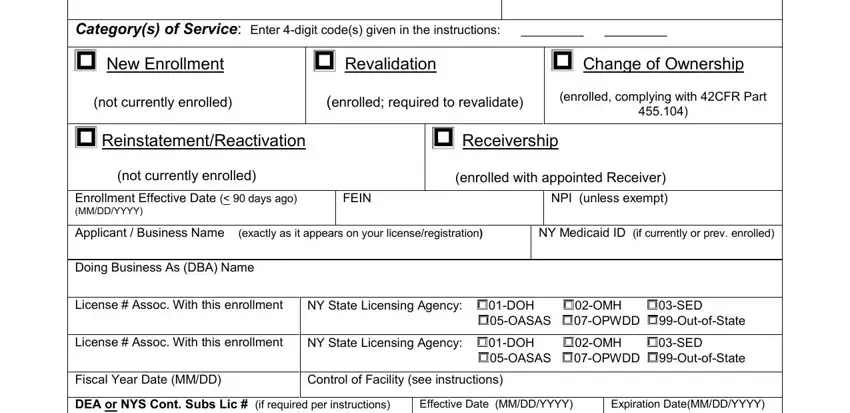
2. Immediately after this part is completed, go on to enter the suitable information in all these: Rensselaer NY, Revalidation, New Enrollment, Categorys of Service Enter digit, enrolled with appointed Receiver, enrolled required to revalidate, Receivership, NPI unless exempt, FEIN, Change of Ownership, enrolled complying with CFR Part, NY Medicaid ID if currently or, Doing Business As DBA Name, License Assoc With this enrollment, and License Assoc With this enrollment.
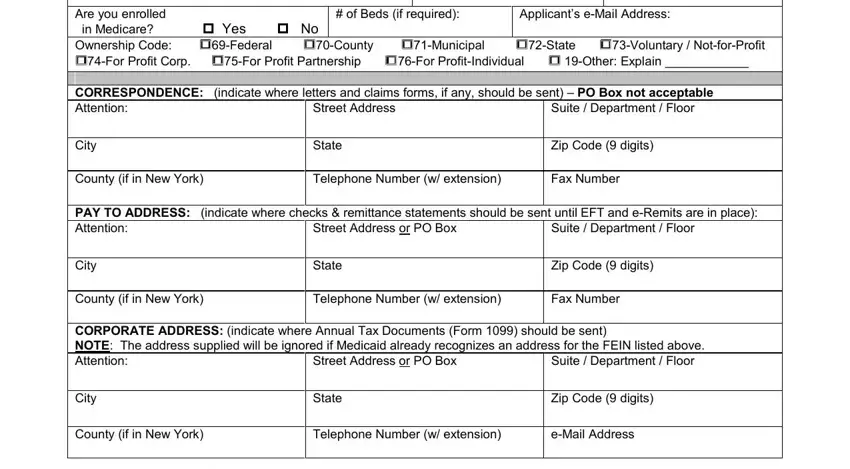
3. Completing of Beds if required, Are you enrolled in Medicare Yes, Applicants eMail Address, Suite Department Floor, Street Address, City, State, Zip Code digits, County if in New York, Telephone Number w extension, Fax Number, PAY TO ADDRESS indicate where, Suite Department Floor, Street Address or, and PO Box is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!
4. To move ahead, this step requires filling out several empty form fields. Examples of these are SERVICE ADDRESS Only if listed on, Street Address PO Box is not, City, State, Zip Code digit, County if in New York, Telephone Number w extension, Fax Number, SERVICE ADDRESS Only if listed on, Street Address PO Box is not, City, State, Zip Code digit, County if in New York, and Telephone Number w extension, which you'll find key to moving forward with this particular form.
5. This document has to be finished by filling in this segment. Below you have a comprehensive set of blank fields that have to be filled out with accurate information in order for your form usage to be faultless: County if in New York, Telephone Number w extension, Fax Number, SERVICE ADDRESS Only if listed on, Street Address PO Box is not, City, State, Zip Code digit, County if in New York, Telephone Number w extension, Fax Number, SERVICE ADDRESS Only if listed on, Street Address PO Box is not, City, and State.
Always be really attentive while filling out State and Fax Number, since this is where many people make mistakes.
Step 3: When you have looked over the details in the document, simply click "Done" to finalize your FormsPal process. Sign up with us today and easily access emedny form 436601, set for downloading. Every last modification you make is handily kept , which enables you to modify the form further when required. FormsPal ensures your information privacy with a secure method that never records or distributes any sort of private information used in the form. Feel safe knowing your documents are kept safe every time you use our editor!