The PDF editor makes it simple to fill out the opm form file. You will be able to make the form easily through these simple steps.
Step 1: First, choose the orange "Get form now" button.
Step 2: Once you have accessed the opm form edit page, you will notice all actions it is possible to take regarding your document at the top menu.
Fill in the opm form PDF by providing the content meant for every single part.
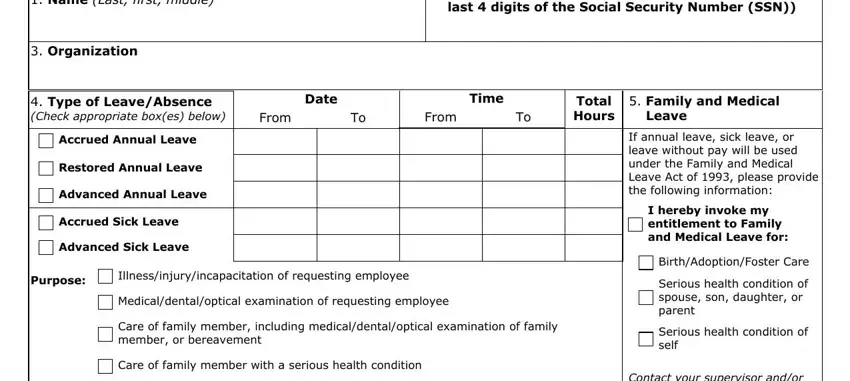
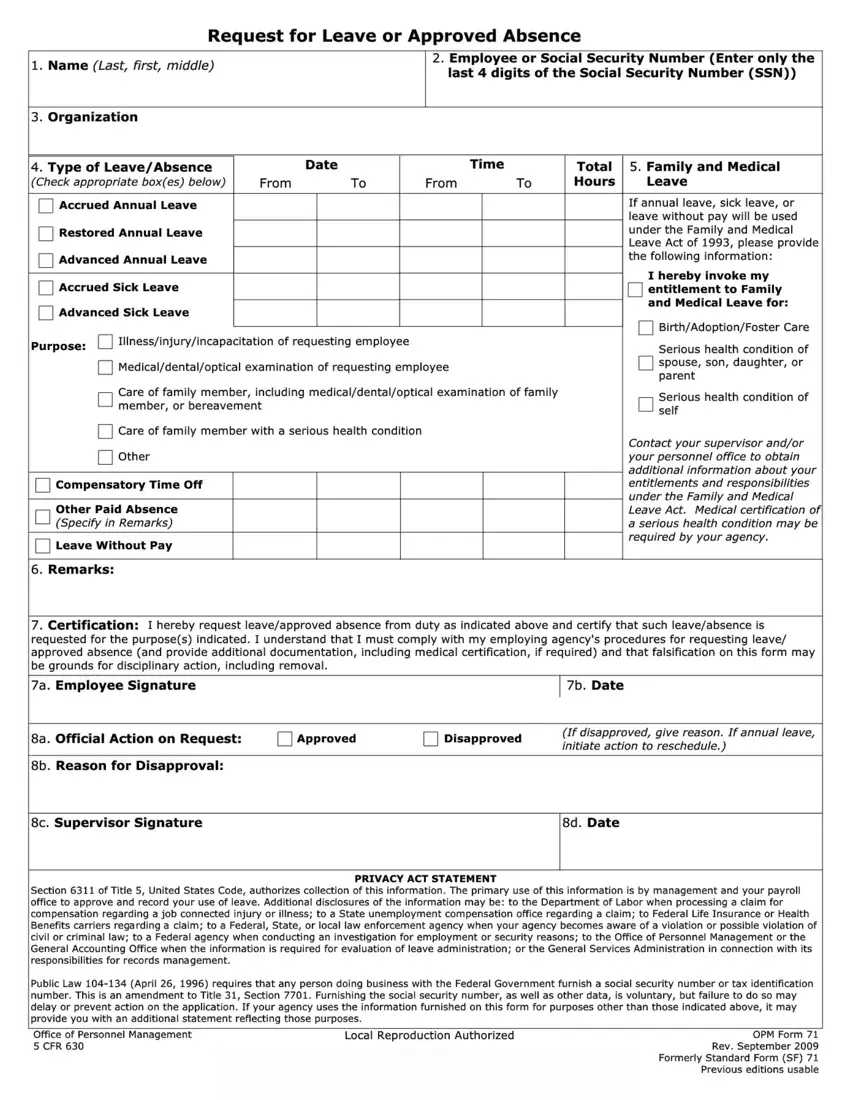
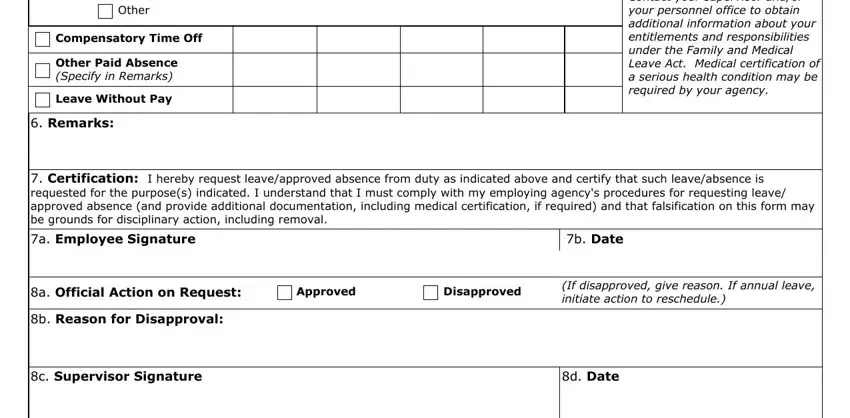
Write down the essential particulars in Other, Compensatory Time Off, Other Paid Absence Specify in, Leave Without Pay, Remarks, Contact your supervisor andor your, Certification I hereby request, a Employee Signature, b Date, a Official Action on Request, Approved, Disapproved, If disapproved give reason If, b Reason for Disapproval, and c Supervisor Signature segment.
Write down any data you are required within the segment Office of Personnel Management, Local Reproduction Authorized, and OPM Form Rev September Formerly.

Step 3: Select "Done". Now you may export your PDF document.
Step 4: Get a duplicate of every single document. It may save you some time and allow you to stay clear of complications as time goes on. Also, your information will not be shared or viewed by us.
