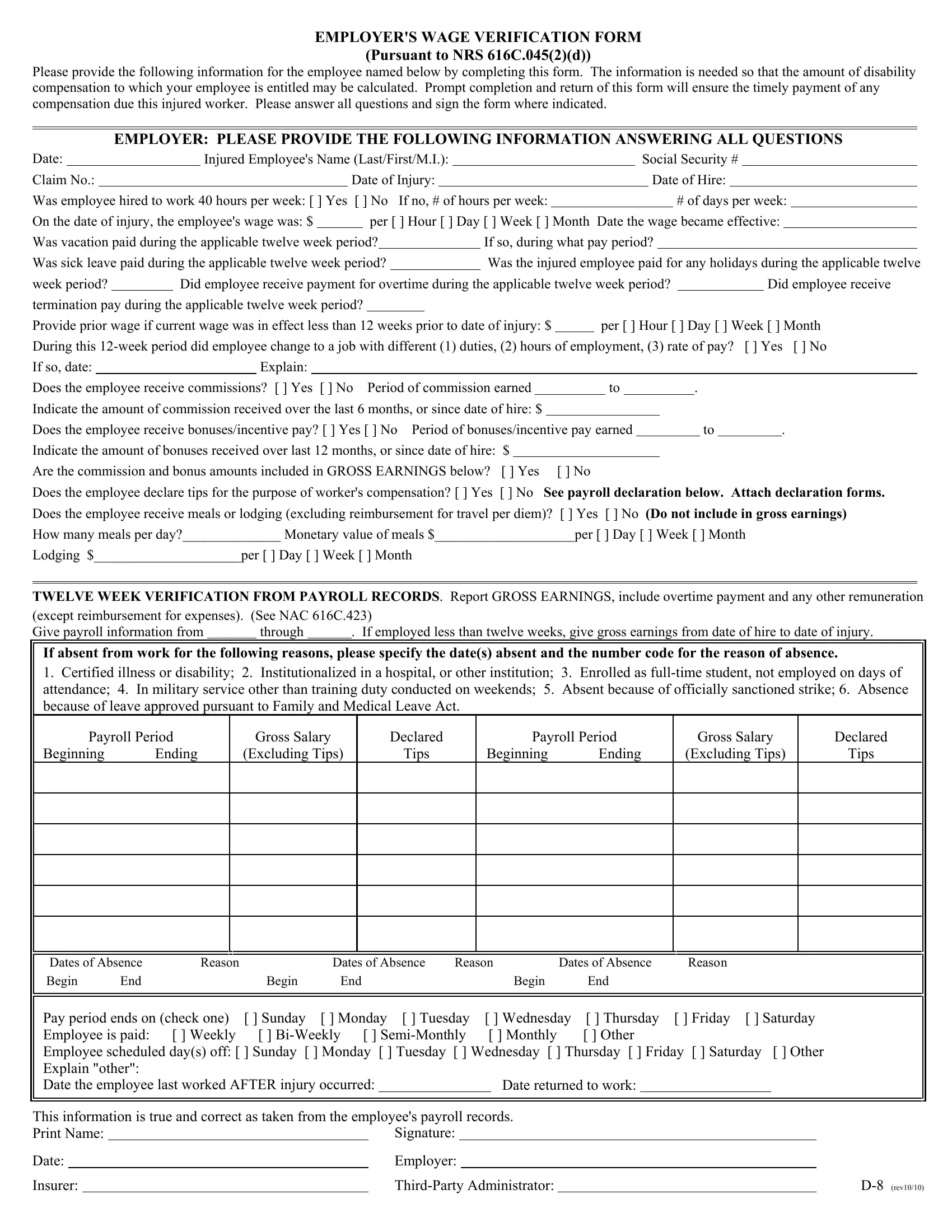
Navigating the complexities of workplace injuries and the associated compensations can be daunting for both employers and employees. Central to this process is the Employer Wage Verification form, a comprehensive document designed under the guidelines provided by the NRS 616C.045(2)(d). Required to be filled out by employers, the form plays a pivotal role in calculating the disability compensation owed to an injured worker. It prompts employers to detail the employee's wage information, hours worked, and any additional earnings such as overtime, bonuses, or commissions. Moreover, it asks for specifics pertaining to the employee's working hours, changes in job duties, or pay rates. Highlighting the significance of timeliness, the form emphasizes the importance of prompt submission to facilitate the timely payment of any due compensation. It encapsulates a range of employer obligations, from verifying the wages over a specified period to accounting for any absences, showcasing the intricate process involved in ensuring injured workers are fairly compensated. This thorough documentation process underscores the commitment to transparency and accuracy in the resolution of compensation claims, ultimately serving as a critical tool in the navigation of worker's compensation procedures.
| Question | Answer |
|---|---|
| Form Name | Employer Wage Verification Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | s pursuant 616c form, 616c employee compensation online, employer wage verification template, wage verification 616c form |
