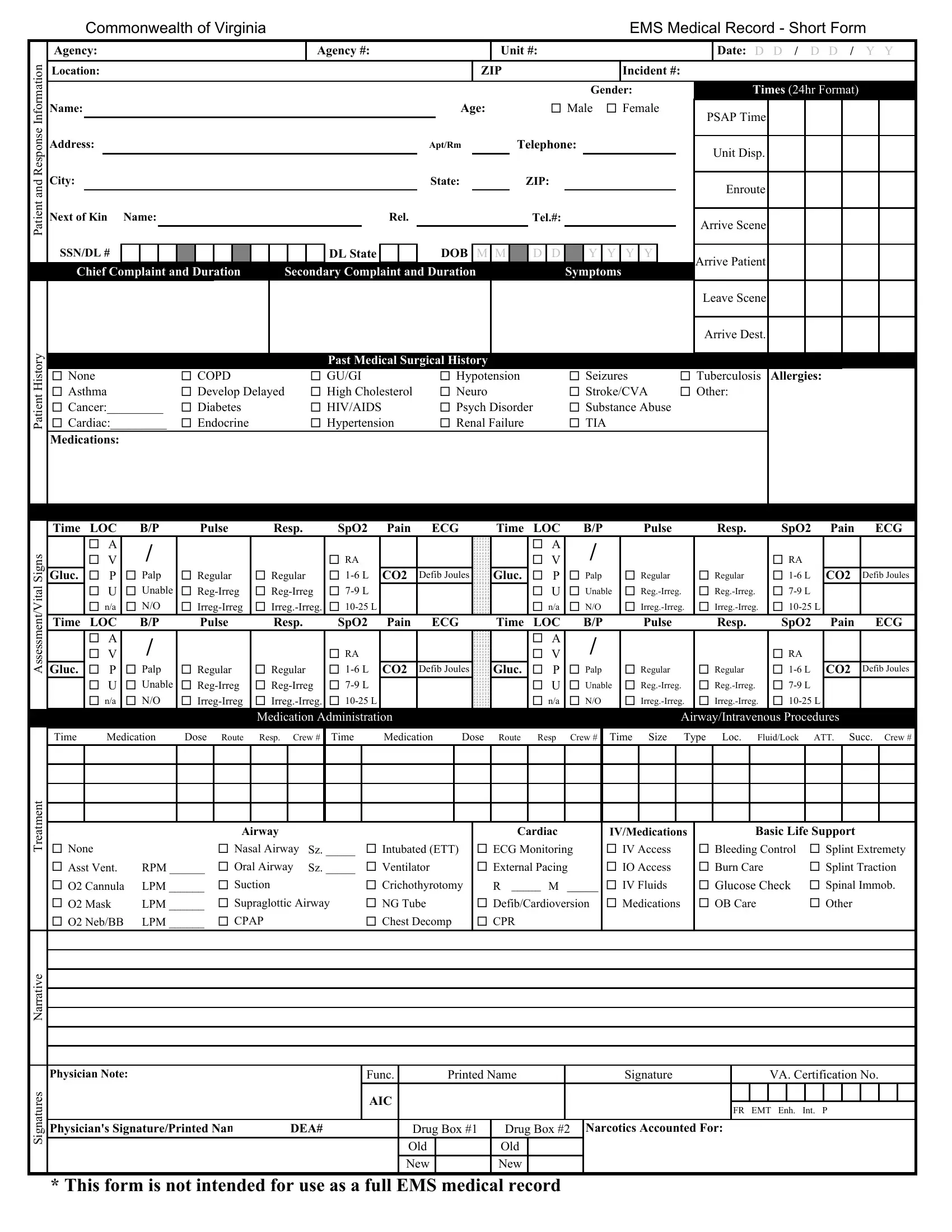
Emergency Medical Services (EMS) teams across the Commonwealth of Virginia rely on the EMS Medical Record - Short Form to accurately document critical patient information during the fast-paced and often chaotic emergency response situations. This comprehensive form captures a wide range of data points essential for the subsequent care and treatment of the patient. It includes identifiers like agency and incident numbers, patient demographics, chief and secondary complaints, detailed symptom chronology, and vital patient history. Additionally, it outlines the response timeline—from the moment the unit is dispatched to the patient's arrival at the destination. The form further delves into a patient's medical history, allergies, medications, and provides a structured section for recording assessment and vital signs multiple times through the course of care. Treatment narratives, medication administration, and advanced procedures such as airway management and intravenous therapies are meticulously logged. Signatures from the attending EMS personnel validate the form, ensuring a traceable and accountable record. This short form, by design, supports not just immediate patient care needs but also serves as an indispensable link in the continuum of care, providing emergency room teams and subsequent caregivers a detailed snapshot of the patient's pre-hospital condition and interventions. While it's clearly stated that this isn't intended to replace a full medical record, its significance in emergent care cannot be overstated, making it a cornerstone document within the EMS documentation suite.
| Question | Answer |
|---|---|
| Form Name | Ems Medical Record Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | Virginia, ECG, irreg, pcr ems |