
Our PDF editor helps make creating documents effortless. It is quite straightforward to manage the [FORMNAME] file. Try out all of these actions if you would like achieve this:
Step 1: Hit the orange "Get Form Now" button on this webpage.
Step 2: Now you can change your genworth independent. This multifunctional toolbar will allow you to insert, remove, transform, and highlight content as well as perform similar commands.
The next few sections will help make up your PDF form:
Fill out the Examination Cal OES, Complete all sections of the form, and Cal OES Revised areas with any data that is requested by the platform.

In the Invoice for Reimbursement for, Law Enforcement Agency, Physical Address, Payment Mailing Address, Exams for victims that are, Date of Examination, Case, Actual Cost of Exam, Reimbursement Requested no more, Exams for victims that have, and Total Requested part, focus on the significant particulars.
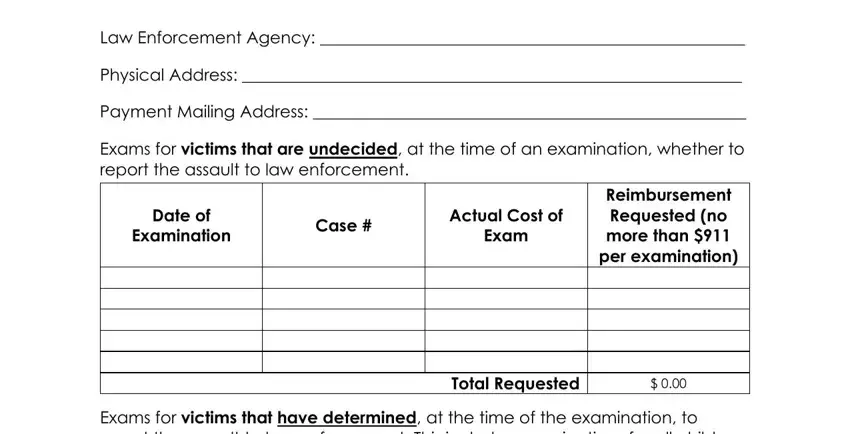
The Reimbursement Requested no more, Total Requested, By submitting this form I certify, Submitted By, Telephone Email, and Cal OES Revised section will be the place to put the rights and obligations of both sides.
Step 3: Select the "Done" button. Now you may upload your PDF file to your gadget. Besides, it is possible to send it via electronic mail.
Step 4: Make sure you keep away from possible future issues by getting minimally 2 duplicates of your document.
