
Any time you want to fill out medical examiners certificate, you don't need to install any sort of applications - just try using our online tool. Our expert team is continuously endeavoring to develop the editor and help it become much easier for clients with its multiple functions. Capitalize on the current progressive possibilities, and discover a heap of unique experiences! If you are looking to get started, this is what it will require:
Step 1: Firstly, access the pdf editor by clicking the "Get Form Button" in the top section of this site.
Step 2: With the help of our state-of-the-art PDF tool, it is possible to do more than merely complete blank form fields. Edit away and make your docs look high-quality with customized text added, or adjust the original content to perfection - all supported by the capability to incorporate stunning photos and sign it off.
With regards to the blanks of this precise form, here's what you need to do:
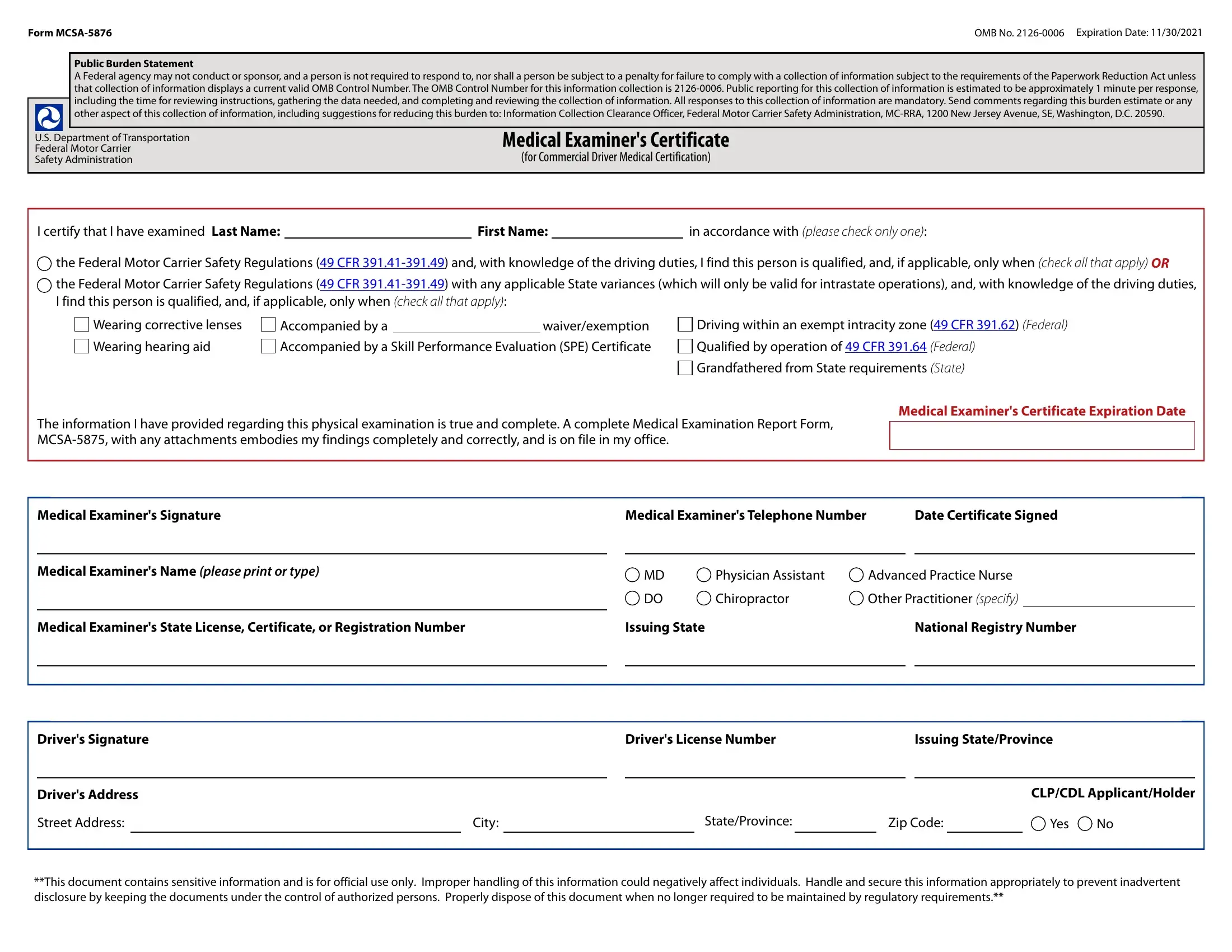
1. For starters, when filling out the medical examiners certificate, beging with the page that contains the next blank fields:
2. Once your current task is complete, take the next step – fill out all of these fields - Drivers Signature, Drivers Address, Street Address, Drivers License Number, Issuing StateProvince, City, StateProvince, Zip Code, Yes, CLPCDL ApplicantHolder, and This document contains sensitive with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!

In terms of Issuing StateProvince and Drivers License Number, ensure you don't make any mistakes in this current part. Those two are the most significant ones in this document.
Step 3: Before finalizing the form, double-check that all blanks have been filled out the correct way. As soon as you believe it is all fine, click “Done." Download the medical examiners certificate the instant you join for a 7-day free trial. Quickly use the form in your FormsPal account page, with any edits and changes being conveniently synced! FormsPal offers protected form completion devoid of data recording or distributing. Feel safe knowing that your information is safe here!