
Our leading developers worked hard to implement the PDF editor we're content to deliver to you. Our application will let you shortly fill out optometry exam form pdf and will save you precious time. You simply need to keep up with the following procedure.
Step 1: Choose the orange button "Get Form Here" on the following website page.
Step 2: Once you've got accessed the editing page optometry exam form pdf, you'll be able to find each of the actions available for the document within the top menu.
You need to provide the next data so you can fill out the document:
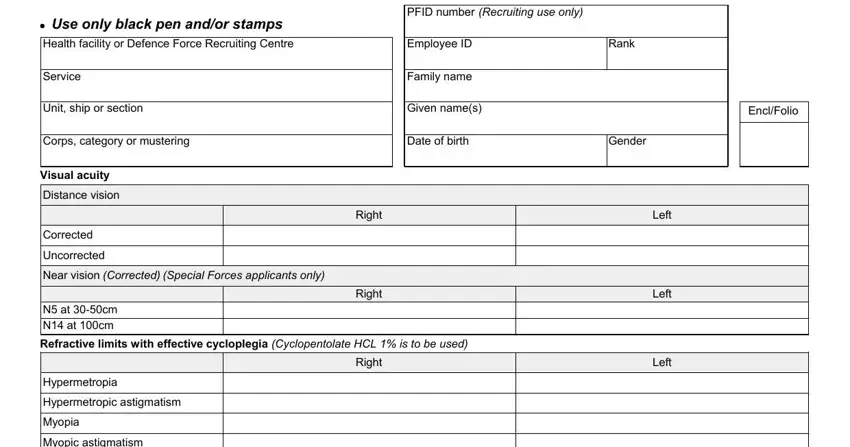
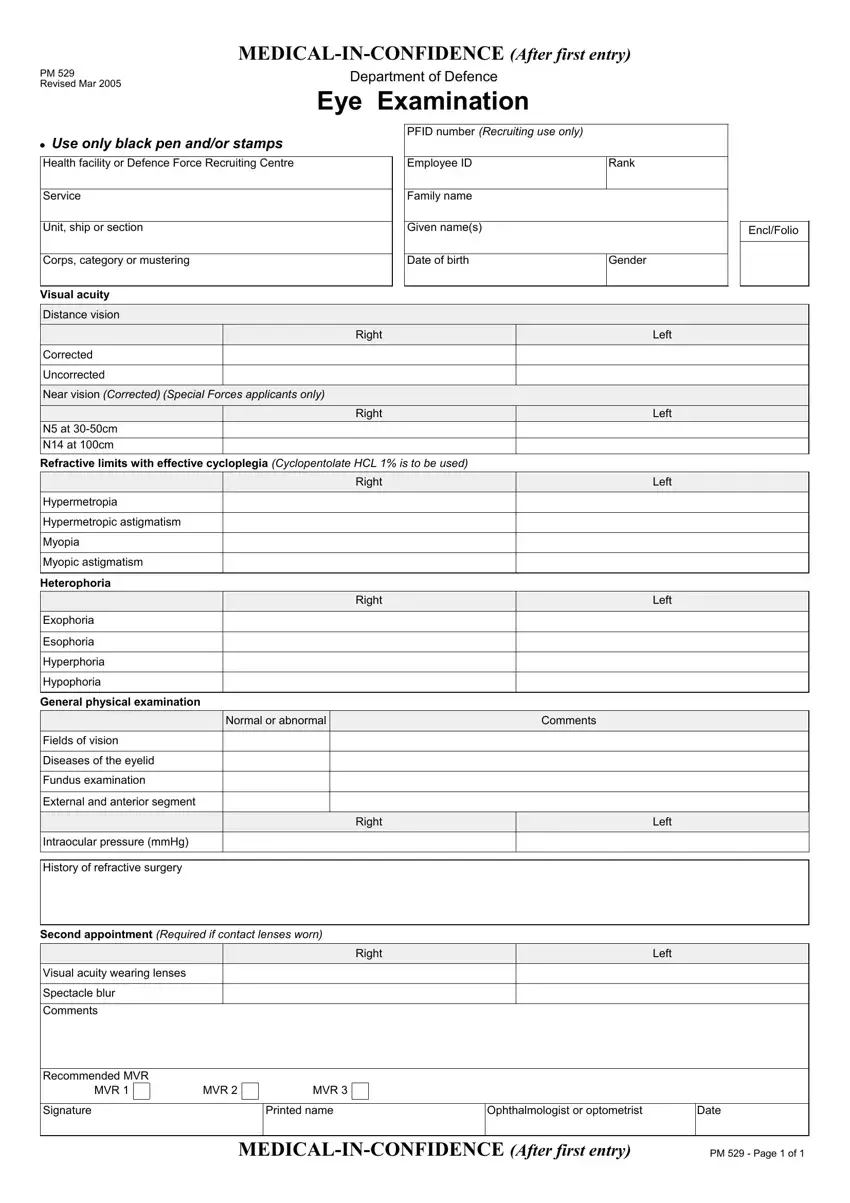
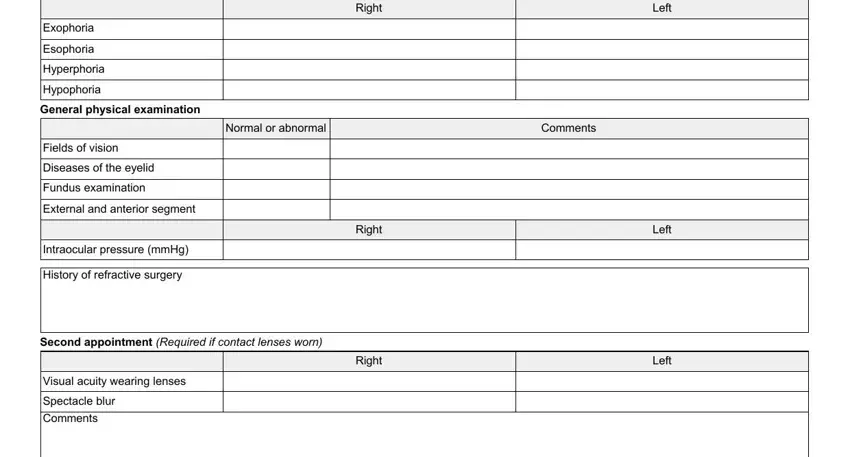
Provide the expected details in the section Right, Normal or abnormal, Comments, Exophoria, Esophoria, Hyperphoria, Hypophoria, General physical examination, Fields of vision, Diseases of the eyelid, Fundus examination, External and anterior segment, Intraocular pressure mmHg, History of refractive surgery, and Right.
You'll be required particular key particulars if you would like fill in the Recommended MVR, MVR, MVR, MVR, Signature, Printed name, Ophthalmologist or optometrist, Date, MEDICALINCONFIDENCE After first, and PM Page of field.

Step 3: As soon as you've selected the Done button, your form is going to be ready for transfer to any electronic device or email address you identify.
Step 4: Make sure to remain away from possible future difficulties by making minimally a pair of copies of your form.
