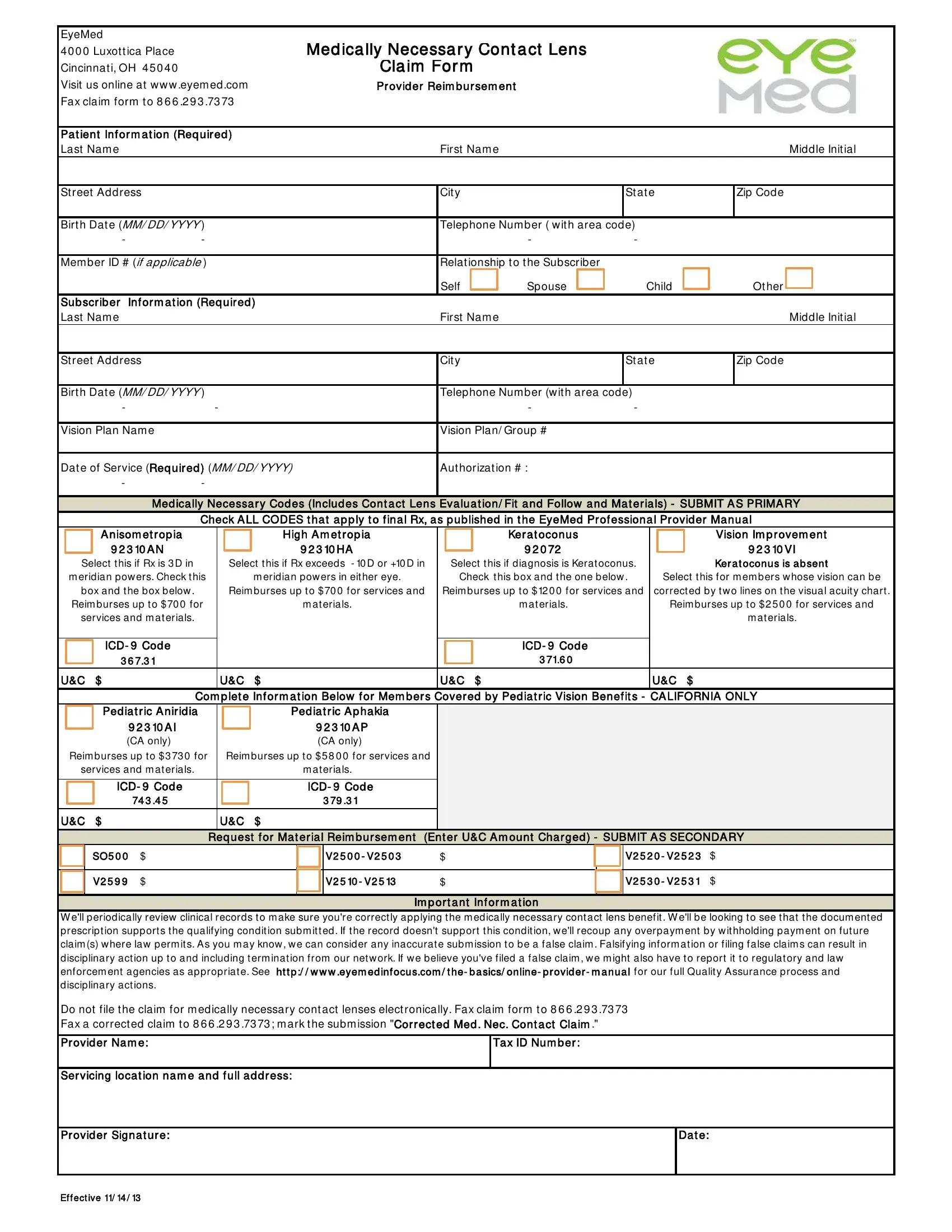
For individuals with specific eye conditions, the accuracy and care in selecting the correct contact lenses are not just a matter of comfort, but a necessity. The EyeMed Medically Necessary Contact Lens Claim Form serves as a critical tool in ensuring these patients receive the medically necessary contact lenses prescribed by their eye care professionals. Centrally located at the Luxottica Place in Cincinnati, OH, this form is designed for eye care providers to claim reimbursement for services rendered and materials provided to patients under specific medical conditions such as Anisometropia, High Ametropia, and Keratoconus, among others. The form outlines detailed patient and subscriber information, the required medical necessity codes that justify the use of such lenses, and the associated reimbursement caps for these services and materials. Additionally, it contains specific sections for pediatric patients within California, reflecting unique requirements for this group. Important information on the submission process highlights the strict adherence to proper documentation and the potential consequences of submitting inaccurate claims, underscoring the importance of precision in every step of the claim process. With the convenient option to fax the completed form, EyeMed simplifies the administrative work for providers while focusing on the broader goal of affording patients the vision correction they medically require.
| Question | Answer |
|---|---|
| Form Name | Eyemed Medically Necessary Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | eyemed medically necessary contacts, eyemed medically online, eyemed lens claim form, pdf80kb form from illinois state pension plan eye med |
