
varicella can be completed online with ease. Simply open FormsPal PDF editing tool to complete the job quickly. FormsPal team is committed to providing you with the best possible experience with our editor by regularly presenting new functions and improvements. Our editor is now much more useful with the latest updates! At this point, working with PDF forms is easier and faster than ever. This is what you'll need to do to get going:
Step 1: Just click on the "Get Form Button" in the top section of this page to launch our pdf editing tool. Here you will find all that is necessary to fill out your file.
Step 2: Using our state-of-the-art PDF file editor, you're able to accomplish more than just fill in blank form fields. Express yourself and make your forms appear great with custom textual content added in, or optimize the file's original input to perfection - all comes along with the capability to insert almost any pictures and sign it off.
It really is an easy task to complete the form using this detailed tutorial! Here's what you should do:
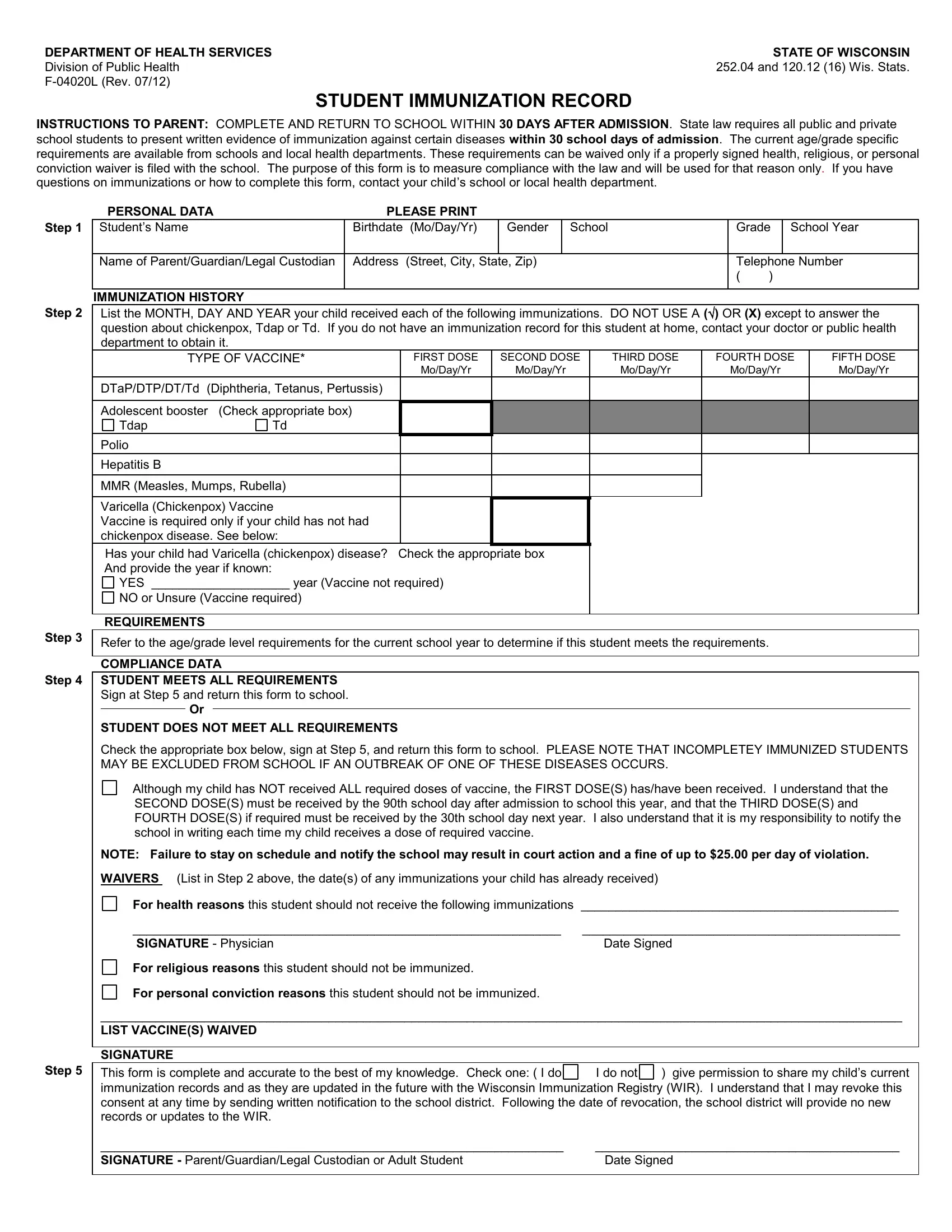
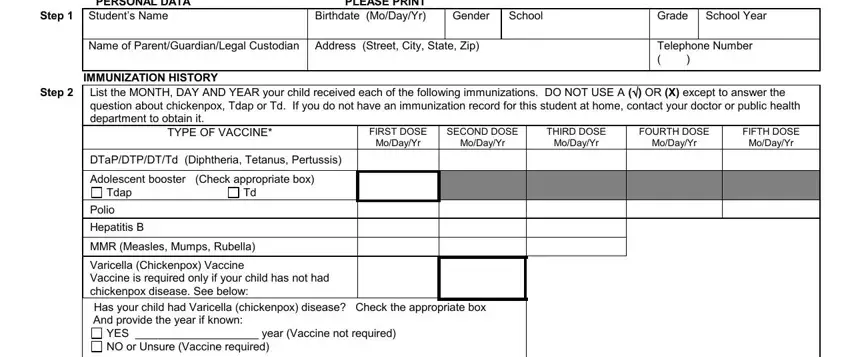
1. The varicella requires certain details to be inserted. Be sure that the subsequent blank fields are finalized:
2. The next step would be to submit these particular blank fields: STUDENT DOES NOT MEET ALL, Although my child has NOT received, SECOND DOSES must be received by, NOTE Failure to stay on schedule, For health reasons this student, SIGNATURE Physician Date Signed, For religious reasons this student, For personal conviction reasons, LIST VACCINES WAIVED SIGNATURE, Step This form is complete and, give permission to share my, and I do not.
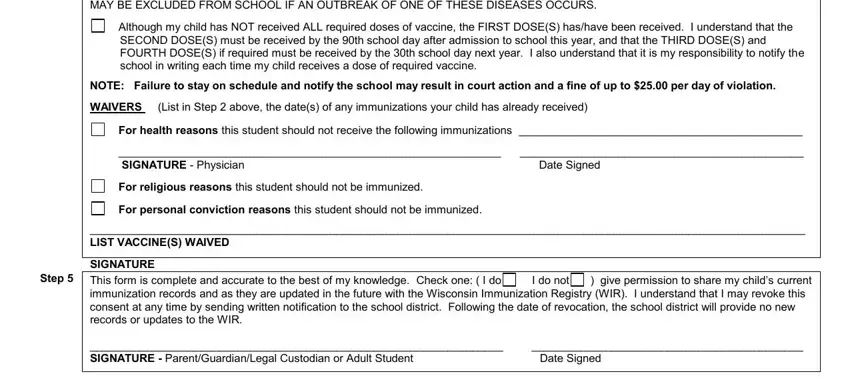
People who work with this document frequently make some mistakes when filling out I do not in this section. Remember to reread whatever you type in here.
Step 3: Revise the information you have inserted in the blank fields and then hit the "Done" button. Acquire the varicella when you sign up at FormsPal for a free trial. Easily access the document within your personal account page, with any edits and adjustments automatically preserved! FormsPal is dedicated to the privacy of all our users; we make sure that all information coming through our tool continues to be secure.