
Once you open the online PDF tool by FormsPal, it is possible to complete or modify fall risk assessments right here. FormsPal team is dedicated to giving you the ideal experience with our tool by continuously releasing new functions and enhancements. With all of these improvements, using our tool gets better than ever! To get the process started, go through these easy steps:
Step 1: Just press the "Get Form Button" above on this webpage to start up our pdf editing tool. Here you will find all that is necessary to fill out your file.
Step 2: As soon as you start the editor, there'll be the document prepared to be completed. Apart from filling out different fields, it's also possible to perform various other actions with the file, such as adding your own words, changing the initial text, inserting illustrations or photos, affixing your signature to the document, and much more.
It will be easy to complete the pdf adhering to our helpful tutorial! Here is what you have to do:
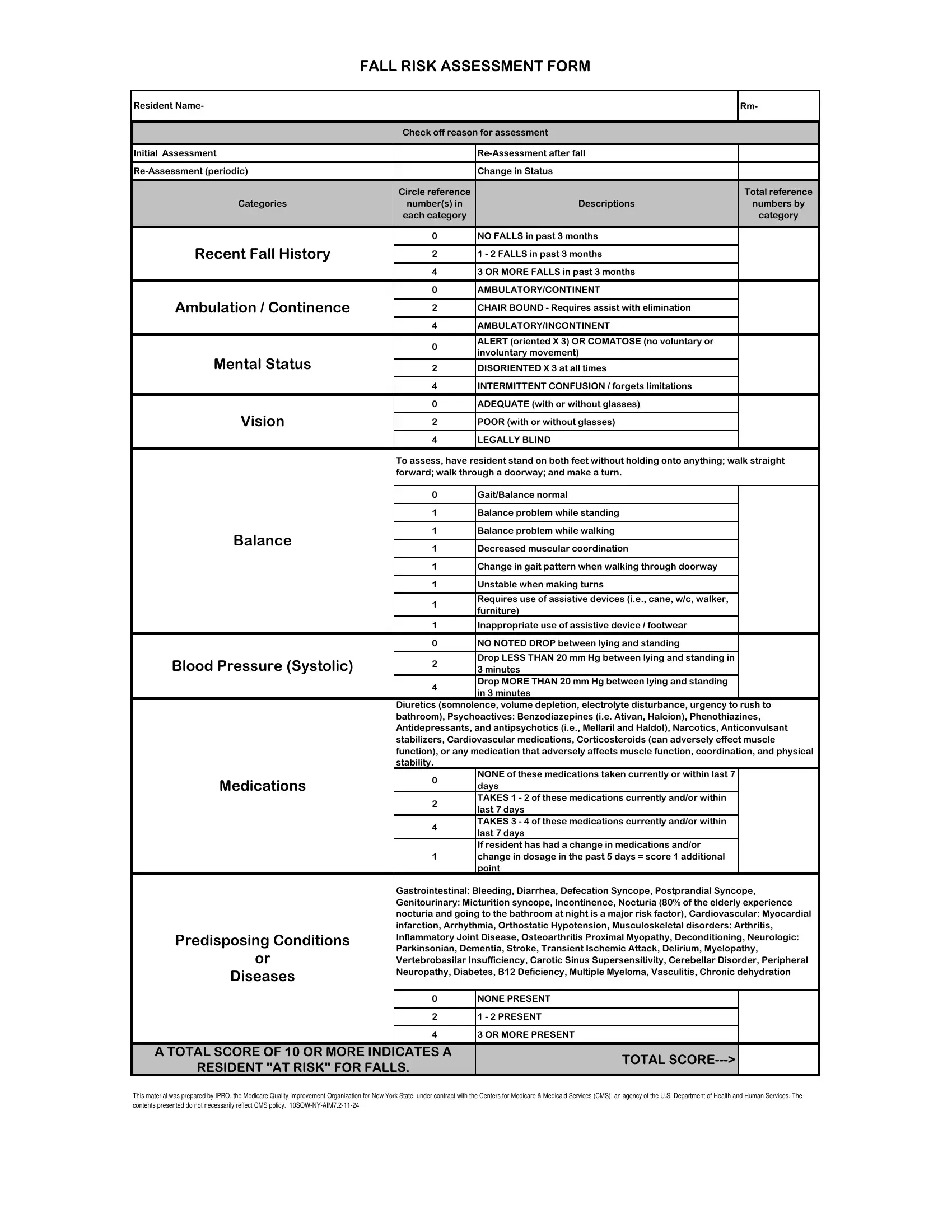
1. While filling out the fall risk assessments, make sure to complete all important blanks within the corresponding part. This will help facilitate the work, allowing your details to be handled quickly and correctly.
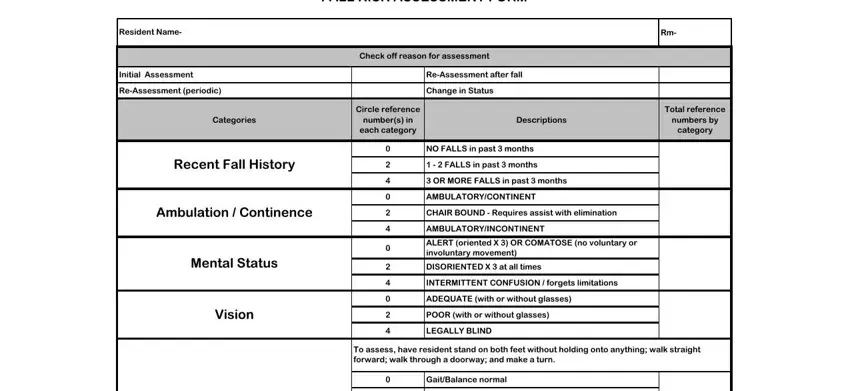
2. Once your current task is complete, take the next step – fill out all of these fields - Balance, Blood Pressure Systolic, Medications, Predisposing Conditions, Diseases, Balance problem while standing, Balance problem while walking, Decreased muscular coordination, Change in gait pattern when, Unstable when making turns, Requires use of assistive devices, Inappropriate use of assistive, NO NOTED DROP between lying and, Drop LESS THAN mm Hg between, and Diuretics somnolence volume with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
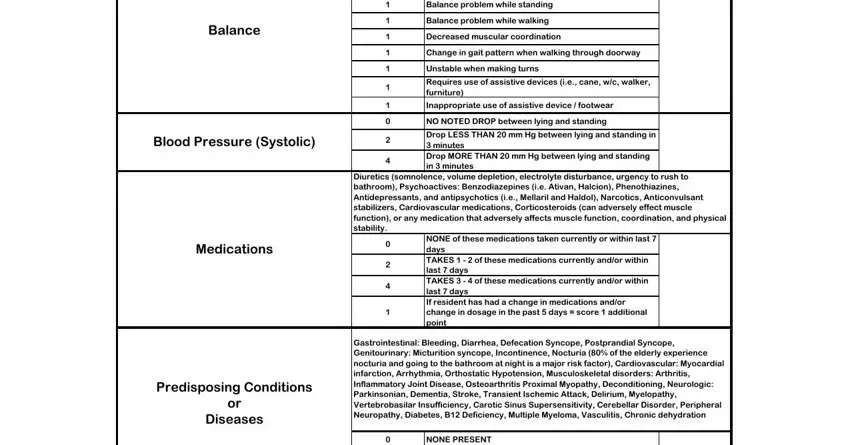
Always be very mindful when completing Predisposing Conditions and Balance, as this is where a lot of people make errors.
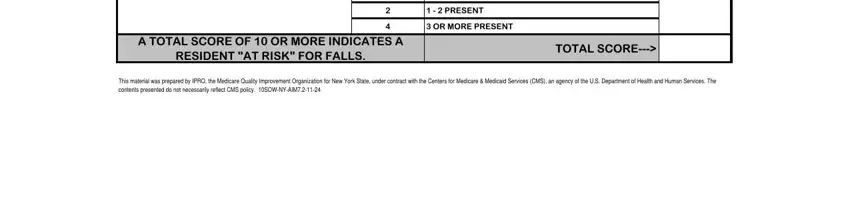
3. The next step will be straightforward - fill out every one of the empty fields in NONE PRESENT, PRESENT, OR MORE PRESENT, A TOTAL SCORE OF OR MORE, RESIDENT AT RISK FOR FALLS, TOTAL SCORE, and This material was prepared by IPRO to complete this segment.
Step 3: After going through your entries, click "Done" and you are done and dusted! Sign up with us today and instantly get access to fall risk assessments, ready for download. Every single edit made is conveniently kept , enabling you to modify the form at a later stage as needed. With FormsPal, it is simple to fill out documents without worrying about personal data leaks or entries getting distributed. Our secure software helps to ensure that your private data is maintained safe.