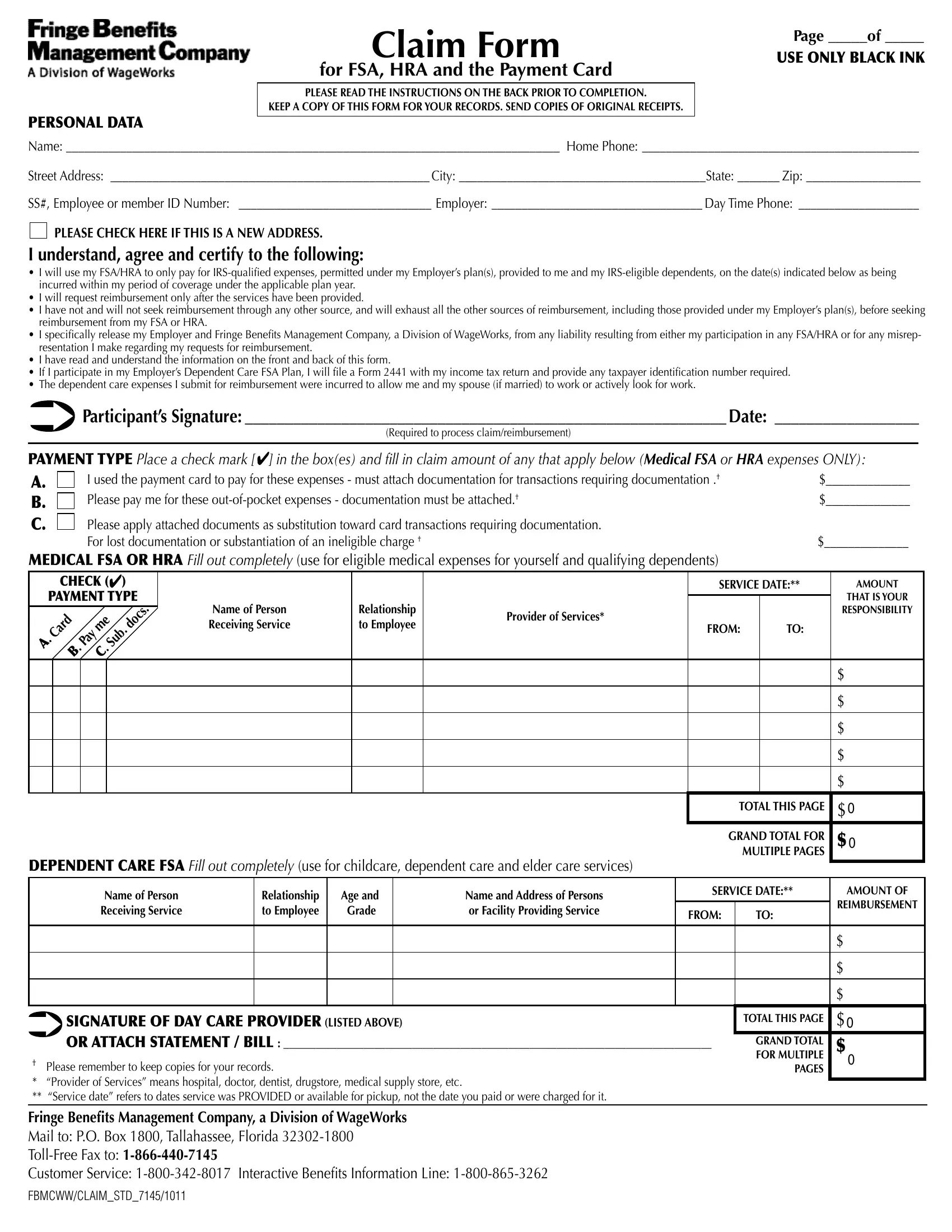
Claim Form |
USE ONLY BLACK INK |
|
Page _____of _____ |
for FSA, HRA and the Payment Card |
|
|
|
PLEASE READ THE INSTRUCTIONS ON THE BACK PRIOR TO COMPLETION. |
|
KEEP A COPY OF THIS FORM FOR YOUR RECORDS. SEND COPIES OF ORIGINAL RECEIPTS. |
|
|
|
UhtlA#ffffffffffffffffffffffffffffffffffffffffffffffffffffffffffffffffffffffffffffffffff##Ovtl#WovulA#ffffffffffffffffffffffffffffffffffffffffffffff
Z{yll{#HkkylzzA##fffffffffffffffffffffffffffffffffffffffffffffffffffff Jp{⦆A#fffffffffffffffffffffffffffffffffffffffffZ{h{lA#fffffff apwA#fffffffffffffffffff
ZZ*3#Ltwsv⦆ll#vy#MITJ#PK#U|tilyA##ffffffffffffffffffffffffffffffffff#Ltwsv⦆lyA##fffffffffffffffffffffffffffffffffff Kh⦆#[ptl#WovulA##ffffffffffffffffffff
PLEASE CHECK HERE IF THIS IS A NEW ADDRESS.
I understand, agree and certify to the following:
ヒ# P#~pss#|zl#t⦆#MZH6OYH#{v#vus⦆#wh⦆#mvy#PYZ4x|hspᅣlk#l⦅wluzlz3#wlytp{{lk#|ukly#t⦆#Ltwsv⦆lyᄏz#wshu/z03#wyv}pklk#{v#tl#huk#t⦆#PYZ4lspnpisl#klwluklu{z3#vu#{ol#kh{l/z0#pukpjh{lk#ilsv~#hz#ilpun#
puj|yylk#~p{opu#t⦆#wlypvk#vm#jv}lyhnl#|ukly#{ol#hwwspjhisl#wshu#⦆lhy5 ヒ# P#~pss#ylx|lz{#ylpti|yzltlu{#vus⦆#hm{ly#{ol#zly}pjlz#oh}l#illu#wyv}pklk5
ヒ# P#oh}l#uv{#huk#~pss#uv{#zllr#ylpti|yzltlu{#{oyv|no#hu⦆#v{oly#zv|yjl3#huk#~pss#l⦅oh|z{#hss#{ol#v{oly#zv|yjlz#vm#ylpti|yzltlu{3#pujs|kpun#{ovzl#wyv}pklk#|ukly#t⦆#Ltwsv⦆lyᄏz#wshu/z03#ilmvyl#zllrpun#
ylpti|yzltlu{#myvt#t⦆#MZH#vy#OYH5
ヒ# P#zwljpᅣjhss⦆#ylslhzl#t⦆#Ltwsv⦆ly#huk#MITJ#myvt#hu⦆#sphipsp{⦆#ylz|s{pun#myvt#lp{oly#t⦆#why{pjpwh{pvu#pu#hu⦆#MZH6OYH#vy#mvy#hu⦆#tpzylwylzlu{h{pvu#P#thrl#ylnhykpun#t⦆#ylx|lz{z#mvy#ylpti|yzltlu{5 ヒ# P#oh}l#ylhk#huk#|uklyz{huk#{ol#pumvyth{pvu#vu#{ol#myvu{#huk#ihjr#vm#{opz#mvyt5
ヒ# Pm#P#why{pjpwh{l#pu#t⦆#Ltwsv⦆lyᄏz#Klwluklu{#Jhyl#MZH#Wshu3#P#~pss#ᅣsl#h#Mvyt#9;;8#~p{o#t⦆#pujvtl#{h⦅#yl{|yu#huk#wyv}pkl#hu⦆#{h⦅wh⦆ly#pklu{pᅣjh{pvu#u|tily#ylx|pylk5 ヒ# [ol#klwluklu{#jhyl#l⦅wluzlz#P#z|itp{#mvy#ylpti|yzltlu{#~lyl#puj|yylk#{v#hssv~#tl#huk#t⦆#zwv|zl#/pm#thyyplk0#{v#~vyr#vy#hj{p}ls⦆#svvr#mvy#~vyr5
Participant’s Signature: ____________________________________________________________ Date: __________________
(Required to process claim/reimbursement)
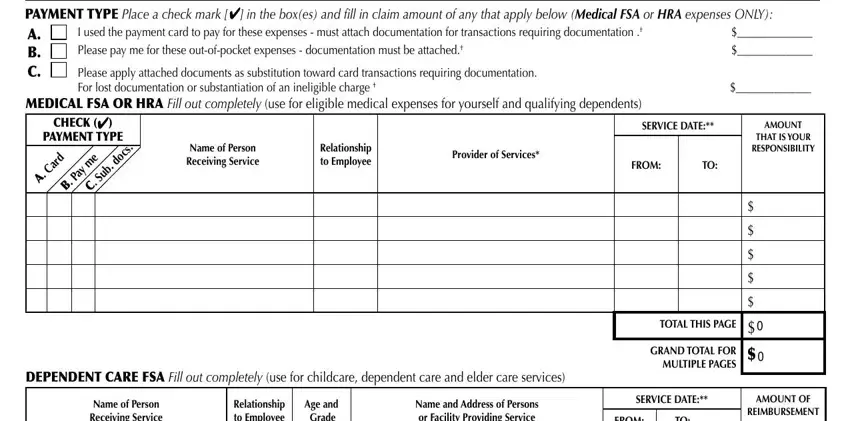
PAYMENT TYPE Place a check mark []#pu#{ol#iv⦅/lz0#huk#ᅣss#pu#jshpt#htv|u{#vm#hu⦆#{oh{#hwws⦆#ilsv~#/MEDICAL FSA or HRA expenses ONLY):
A. +ffffffffffffff##P#|zlk#{ol jhyk#{v#wh⦆#mvy#{olzl#l⦅wluzlz#4#t|z{#h{{hjo#kvj|tlu{h{pvu#mvy#{yhuzhj{pvuz#ylx|pypun#kvj|tlu{h{pvu#5†
B. +ffffffffffffff##Wslhzl#wh⦆#tl#mvy#{olzl#v|{4vm4wvjrl{#l⦅wluzlz#4#kvj|tlu{h{pvu#t|z{#il#h{{hjolk5†
C. |
|
+ffffffffffffff##Wslhzl#hwws⦆#h{{hjolk#kvj|tlu{z#hz#z|iz{p{|{pvu#{v~hyk#jhyk#{yhuzhj{pvuz#ylx|pypun#kvj|tlu{h{pvu5#Mvy#svz{#kvj|tlu{h{pvu#vy### |
|
|
# |
z|iz{hu{ph{pvu#vm#hu#pulspnpisl#johynl#† |
MEDICAL FSA OR HRA Fill out completely /|zl#mvy#lspnpisl#tlkpjhs#l⦅wluzlz#mvy#⦆v|yzlsm#huk#x|hspm⦆pun#klwluklu{z0
|
|
CHECK ( |
) |
|
|
|
SERVICE DATE:** |
AMOUNT |
|
PAYMENT TYPE |
|
|
|
|
|
|
|
|
|
THAT IS YOUR |
|
|
|
|
|
|
|
|
. |
Name of Person |
Relationship |
Provider of Services* |
|
|
RESPONSIBILITY |
|
Card |
|
|
me |
|
.docs |
Receiving Service |
to Employee |
FROM: |
TO: |
|
|
|
|
|
|
|
. |
|
|
Pay |
|
|
Sub |
|
|
|
|
|
|
A |
|
|
. . |
|
|
|
|
|
|
|
|
|
|
B |
|
C |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
$ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
$ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
$ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
$ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
$ |
|
|
|
|
|
|
|
|
|
|
|
|
TOTAL THIS PAGE |
$ |
|
|
|
|
|
|
|
|
|
|
|
|
GRAND TOTAL FOR |
$ |
|
|
|
|
|
|
|
|
|
|
|
|
|
MULTIPLE PAGES |
|
DEPENDENT CARE FSA Fill out completely /|zl#mvy#jopskjhyl3#klwluklu{#jhyl#huk#lskly#jhyl#zly}pjlz0 |
|
|
|
|
|
|
|
|
|
Name of Person |
Relationship |
Age and |
Name and Address of Persons |
SERVICE DATE:** |
AMOUNT OF |
|
|
|
|
|
|
|
|
REIMBURSEMENT |
|
|
|
|
|
Receiving Service |
to Employee |
Grade |
or Facility Providing Service |
FROM: |
TO: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
$
$
$
SIGNATURE OF DAY CARE PROVIDER (LISTED ABOVE) |
TOTAL THIS PAGE |
$ |
OR ATTACH STATEMENT / BILL : ________________________________________________________________________________ |
GRAND TOTAL |
$ |
†# Wslhzl#yltltily#{v#rllw#jvwplz#mvy#⦆v|y#yljvykz5 |
FOR MULTIPLE |
PAGES |
|
1## ᄌWyv}pkly#vm#Zly}pjlzᄍ#tlhuz#ovzwp{hs3#kvj{vy3#klu{pz{3#ky|nz{vyl3#tlkpjhs#z|wws⦆#z{vyl3#l{j5 |
|
|
|
|
11##ᄌZly}pjl#kh{lᄍ#ylmlyz#{v#kh{lz#zly}pjl#~hz#WYV]PKLK#vy#h}hpshisl#mvy#wpjr|w3#uv{#{ol#kh{l#⦆v|#whpk#vy#~lyl#johynlk#mvy#p{5 |
|
|
FBMC
Thps#{vA#W5V5#Iv⦅#8?773#[hsshohzzll3#Msvypkh#:9:7948?77 [vss4Myll#Mh⦅#{vA#1-866-923-6318
J|z{vtly#Zly}pjlA#84?774:;94?78>##Pu{lyhj{p}l#Ilulᅣ{z#Pumvyth{pvu#SpulA#84?774?=<4:9=9
FBMC/CLAIM_PRM_6318/0408
IMPORTANT INFORMATION FOR REIMBURSEMENT
(TO AVOID DELAYS, PLEASE READ THESE INSTRUCTIONS CAREFULLY.)
IMPORTANT REQUIREMENTS & INFORMATION /uv{#mvssv~pun#{olzl#ylx|pyltlu{z#th⦆#jh|zl#⦆v|y#jshpt#{v#il#ylqlj{lk0 ヒ# Jvtwsl{l#hss#spulz#pu#{ol#Wlyzvuhs#Kh{h#Zlj{pvu5
ヒ# \zl#ishjr#pur#vus⦆5
ヒ# Kv#uv{#|zl#opnospno{#thyrlyz#vu#⦆v|y#jshpt#mvyt#vy#kvj|tlu{h{pvu#/~l#zjhu#hss#kvj|tlu{z05 ヒ##`v|y#MITJ#PK#*#jhu#il#vi{hpulk#vu#v|y#~li#zp{l#h{#www.myFBMC.com#hm{ly#svnpu5#
ヒ# Z|itp{#jvwplz#vm#pu}vpjlz3#z{h{ltlu{z3#ipssz3#yljlpw{z3#vy#LVI#pu#{ol#zhtl#vykly#hz#spz{lk#vu#{ol#jshpt#mvyt5# ヒ# Jylkp{#jhyk#yljlpw{z#huk#jhujlslk#joljrz#jhuuv{#il#|zlk#{v#hwwyv}l#⦆v|y#jshpt5
ヒ# Hjjv|u{#ovskly#t|z{#zpnu#huk#kh{l#{ol#jshpt#mvyt5 ヒ# Tvyl#mvytz#hyl#h}hpshisl#h{#www.myFBMC.com5 ヒ# H{{hjo#hkkp{pvuhs#zoll{#mvy#tvyl#p{ltz6spulz5
ヒ# Yl{hpu#h#jvw⦆#vm#⦆v|y#jshpt#mvyt/z0#huk#hss#kvj|tlu{h{pvu#mvy#⦆v|y#yljvykz5
DOCUMENTATION REQUIREMENTS:
Medical Flexible Spending Account (MFSA) or Health Reimbursement Arrangement (HRA)#kvj|tlu{h{pvu#t|z{#pujs|kl#{ol#mvssv~punA ヒ# Kh{l#zly}pjl/z0#~lyl#yljlp}lk#/uv{#uljlzzhyps⦆#zhtl#hz#kh{l#whpk0
ヒ# `v|y#jvz{#mvy#{ol#zly}pjl/z05#[v{hs#htv|u{#{oh{#pz#⦆v|y#ylzwvuzpipsp{⦆5
ヒ# [⦆wl#vm#Zly}pjl/z0#/⦅4yh⦆3#vmᅣjl#}pzp{3#wylzjypw{pvu#ky|n#uhtl#vy#v}ly4{ol4jv|u{ly#p{lt#l{j50
ヒ# Uhtl#vm#wlyzvu#yljlp}pun#zly}pjlz#/{opz#t|z{#il#{ol#hjjv|u{#ovskly3#zwv|zl3#vy#PYZ#lspnpisl#klwluklu{05 ヒ# Hu#LVI#jhu#il#z|itp{{lk#mvy#pu#spl|#vm#h#z{h{ltlu{#vy#ipss5
ヒ# OYHz#4#⦆v|#t|z{#z|itp{#hu#LVI#mvy#hu⦆#tlkpjhs#zly}pjlz#yljlp}lk5#Zll#luyvsstlu{#n|pkl#mvy#hu⦆#hkkp{pvuhs#ᅣspun#ylx|pyltlu{z5
Orthodontics – [ol#mvssv~pun#pz#ylx|pylkA
ヒ# H#~yp{{lu#z{h{ltlu{#myvt#{ol#{ylh{pun#klu{pz{6vy{ovkvu{pz{#zov~pun#{ol#{⦆wl#huk#kh{l#{ol#zly}pjl#puj|yylk3#{ol#uhtl#vm#{ol#lspnpisl#
pukp}pk|hs#yljlp}pun#{ol#zly}pjl#huk#{ol#jvz{#mvy#{ol#zly}pjl#huk
ヒ# H#jvw⦆#vm#{ol#wh{plu{ᄏz#jvu{yhj{#~p{o#{ol#klu{pz{6vy{ovkvu{pz{#mvy#{ol#vy{ovkvu{ph#{ylh{tlu{#/vus⦆#ylx|pylk#pm#h#why{pjpwhu{#ylx|lz{z#
ylpti|yzltlu{#mvy#{ol#{v{hs#wyvnyht#jvz{#zwylhk#v}ly#h#wlypvk#vm#{ptl05# Note:#Ylpti|yzltlu{#vm#{ol#m|ss#vy#pup{phs#wh⦆tlu{#htv|u{#th⦆#vus⦆#vjj|y#k|ypun#{ol#wshu#⦆lhy#pu#~opjo#{ol#iyhjlz#hyl#ᅣyz{#puz{hsslk5#
Dependent Care Flexible Spending Account (DCFSA)
ヒ# Pm#{ol#wlyzvuhs#kh{h#zlj{pvu#huk#{ol#klwluklu{#jhyl#zlj{pvu#hyl#jvtwsl{lk#pu#{olpy#lu{pyl{⦆#huk#{ol#mvyt#ohz#illu#zpnulk#i⦆#⦆v|yzlsm#huk#
⦆v|y#kh⦆#jhyl3#uv#m|y{oly#kvj|tlu{h{pvu#pz#ullklk5
ヒ# Pu#spl|#vm#{ol#wyv}pkly#zpnuh{|yl3#⦆v|#jhu#z|itp{#h#z{h{ltlu{3#pu}vpjl#vy#ipss#{oh{#zov~z#{ol#uhtl#huk#hkkylzz#vm#{ol#wyv}pkly3#ilnpuupun#
huk#lukpun#kh{lz#vm#{ol#wyv}pklk#zly}pjlz3#{ol#jvz{#vm#zly}pjl/z03#huk#{ol#uhtl#vm#{ol#lspnpisl#klwluklu{/z05
ヒ# Jshpt#ylx|lz{z#mvy#t|s{pwsl#tvu{oz#~pss#il#wyvyh{lk#huk#p{ltp。lk#ihzlk#vu#{ol#u|tily#vm#tvu{oz#spz{lk5#Wh⦆tlu{#~pss#il#pzz|lk#hm{ly#{ol#
luk#vm#lhjo#tvu{o#mvy#~opjo#zly}pjlz#~lyl#puj|yylk3#ihzlk#vu#{ol#h}hpshisl#ihshujl#pu#⦆v|y#hjjv|u{5
ヒ# Lk|jh{pvuhs#l⦅wluzlz#puj|yylk#mvy#h#jopsk#pu#rpuklynhy{lu#huk#|w#hyl#uv{#ylpti|yzhisl5#[ol#jvz{#vm#klwluklu{#jhyl#ilmvyl#huk#hm{ly#zjovvs#
pz#ylpti|yzhisl5
ヒ# L⦅wluzlz#z|jo#hz#{|p{pvu3#ylnpz{yh{pvu#mllz3#hj{p}p{⦆#mllz3#ivvrz3#z|wwsplz#huk#tlhsz#hyl#uv{#ylpti|yzhisl5
Special Requirements – Pu#hkkp{pvu#{v#{ol#kvj|tlu{h{pvu#uv{lk#hiv}l3#zvtl#zly}pjlz#ylx|pyl#hkkp{pvuhs#kvj|tlu{h{pvu#z|jo#hz#h#Sl{{ly#vm# Tlkpjhs#Ullk3#h#Jhwp{hs#L⦅wluzl#^vyrzoll{3#vy#h#Wlyzvuhs#\zl#Z{h{ltlu{5#Wslhzl#}pzp{#www.myFBMC.com mvy#jvwplz#huk#klzjypw{pvu#vm#|zl5
Toll-Free Fax to: 1-866-923-6318
Mail to:#Mypunl#Ilulᅣ{z#Thuhnltlu{#Jvtwhu⦆#/MITJ03#W5V5#Iv⦅#8?773#[hsshohzzll3#MS#:9:7948?77
Pu{lyhj{p}l#Ilulᅣ{z#Pumvyth{pvu#SpulA#84?774?=<4:9=9
]pzp{#www.myFBMC.com#mvy#mylx|lu{s⦆#hzrlk#x|lz{pvuz3#hjjv|u{#ihshujlz3# kvj|tlu{h{pvu#ylx|pyltlu{z#mvy#jhyk#{yhuzhj{pvuz3#huk#mvytz5