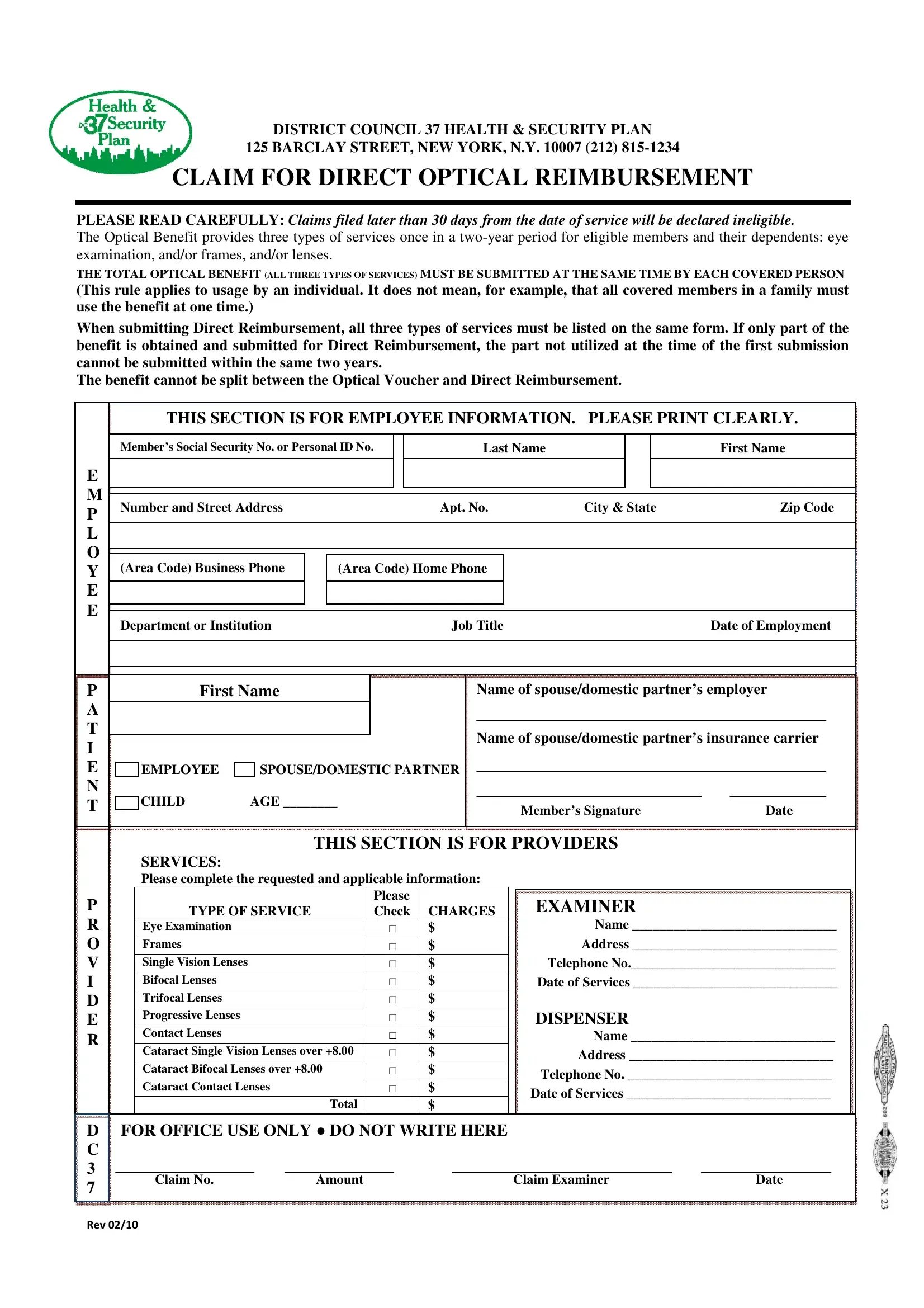
The Claim for Optical Reimbursement form (also known as the DC 37 eye voucher or optical voucher) is the official document District Council 37 Health and Security Plan members use to request direct payment for vision care costs paid out of pocket. Unlike the Optical Voucher benefit, Direct Reimbursement requires you to pay first and then submit this form to recover eligible costs.
Eligibility. Active DC 37 members and their eligible dependents enrolled in the District Council 37 Health and Security Plan may use this form. You cannot split the benefit between the Optical Voucher and Direct Reimbursement options for the same covered individual within the same two-year benefit period.
Covered Services. The plan covers three categories of optical services within any two-year benefit period per covered person: (1) a comprehensive eye examination by a licensed examiner, (2) prescription frames, and (3) corrective lenses. Covered lens types include single vision, bifocal, trifocal, progressive lenses, contact lenses, and cataract lens replacements. All three service types must be claimed together in one submission.
Submission Rules. Claims must be filed within 30 days of the date of service. Late submissions may be denied. Submit one separate form per covered individual if multiple family members need to claim benefits in the same period. Mail the completed form along with itemized receipts to your plan administrator.
Required Information. Complete the employee section (name, address, member ID, and plan number) and the provider section (provider name, address, telephone, type of service, and total charges for each service). Leave the "For Office Use Only" area blank. Review all fields before mailing to avoid processing delays. For related forms, see the Blue Vision Claim Form and the health insurance claim form available at FormsPal.
| Question | Answer |
|---|---|
| Form Name | Claim For Optical Reimbursement Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | dc 37 vision voucher, optical reimbursement form, optical voucher, dc37 voucher request form |