
Handling PDF files online is certainly a breeze with our PDF editor. You can fill out nysna vision benefits here within minutes. In order to make our tool better and simpler to work with, we consistently implement new features, bearing in mind suggestions from our users. It just takes a few easy steps:
Step 1: Hit the orange "Get Form" button above. It's going to open our pdf editor so that you can start filling out your form.
Step 2: This tool lets you change most PDF forms in a variety of ways. Modify it by writing customized text, correct what is originally in the document, and place in a signature - all doable in no time!
This document requires particular data to be filled in, so you must take your time to provide exactly what is asked:
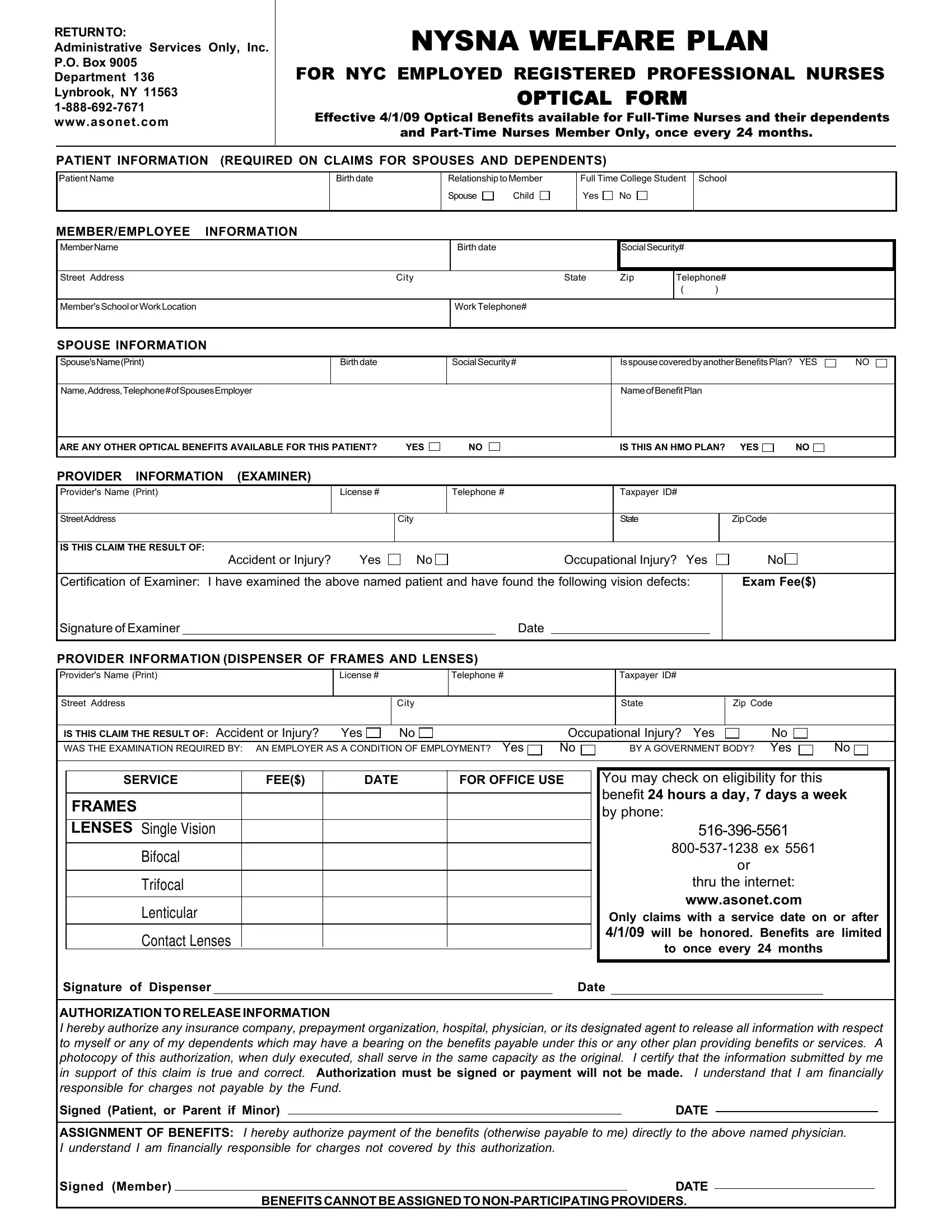
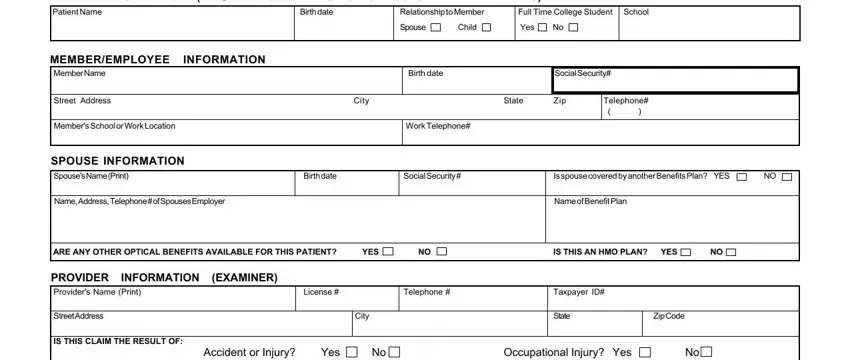
1. The nysna vision benefits will require certain information to be entered. Ensure the next blank fields are complete:
2. Right after completing the previous step, head on to the subsequent step and fill in all required particulars in these blanks - Certification of Examiner I have, Signature of Examiner, Date, PROVIDER INFORMATION DISPENSER OF, License, Telephone, Taxpayer ID, Street Address, City, State, Zip Code, IS THIS CLAIM THE RESULT OF, Occupational Injury Yes, BY A GOVERNMENT BODY Yes, and SERVICE.
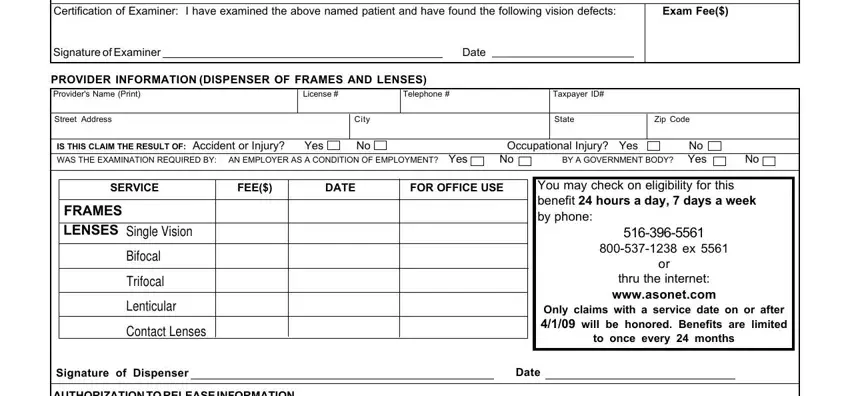
People generally make some errors while filling in Occupational Injury Yes in this section. Don't forget to double-check what you enter here.
3. Completing AUTHORIZATION TO RELEASE, Signed Patient or Parent if Minor, DATE, ASSIGNMENT OF BENEFITS I hereby, Signed Member, DATE, and BENEFITS CANNOT BE ASSIGNED TO is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!

Step 3: Spell-check all the information you've entered into the blanks and then click the "Done" button. Right after creating afree trial account with us, you'll be able to download nysna vision benefits or send it through email at once. The file will also be easily accessible in your personal account with your each modification. FormsPal guarantees risk-free document tools with no personal data record-keeping or distributing. Feel safe knowing that your information is safe here!