This PDF editor makes it simple to fill out documents. You won't need to undertake much to change chi franciscan financial aid form forms. Basically stick to all of these actions.
Step 1: The first thing will be to select the orange "Get Form Now" button.
Step 2: You can find all of the options which you can take on the document after you've entered the wwww chihealth com financial assistance editing page.
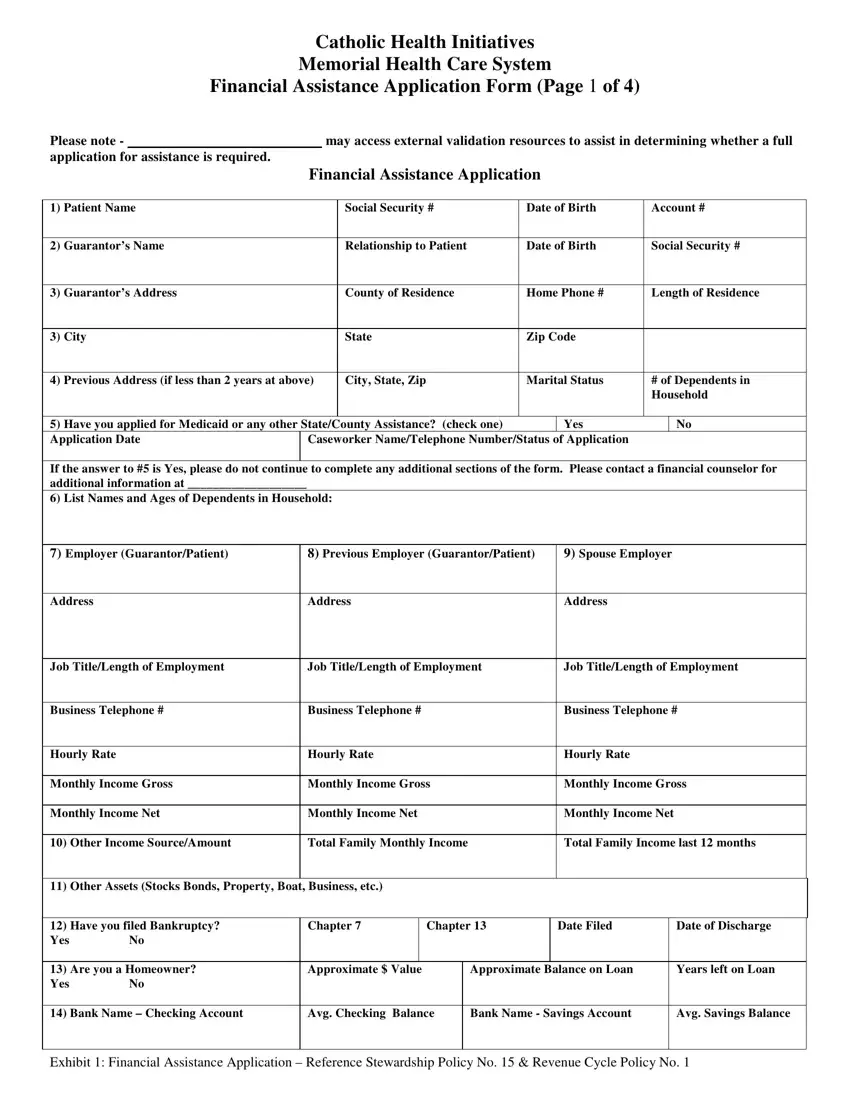
Fill out the wwww chihealth com financial assistance PDF and provide the content for every area:
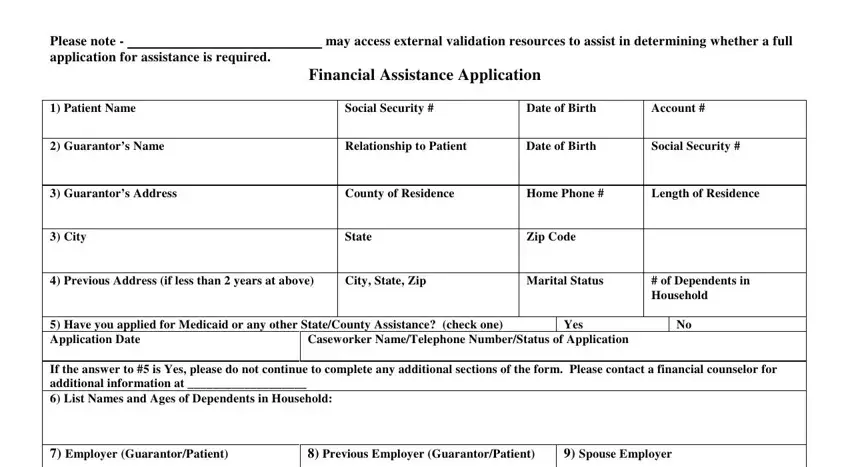
Type in the required particulars in the space Address, Address, Address, Job TitleLength of Employment, Job TitleLength of Employment, Job TitleLength of Employment, Business Telephone, Business Telephone, Business Telephone, Hourly Rate, Hourly Rate, Hourly Rate, Monthly Income Gross, Monthly Income Gross, and Monthly Income Gross.
The application will ask you to give some key info to easily fill out the area Are you a Homeowner Yes No, Approximate Value, Approximate Balance on Loan, Years left on Loan, Bank Name Checking Account, Avg Checking Balance, Bank Name Savings Account, Avg Savings Balance, and Exhibit Financial Assistance.

The Catholic Health Initiatives, Model, Model, Model, Model, Year, Pymt Amount, Year, Pymt Amount, Year, Pymt Amount, Year, Pymt Amount, Balance Due, and Balance Due space is the place where all sides can indicate their rights and responsibilities.
Fill in the template by looking at the next fields: MEDICATION LIFE INSURANCE MEDICAL, Monthly Payment, AUTO INS OTHER OTHER, Monthly Payment, School Loans List Other Expenses, FOOD UTILITIES GAS CAR TOTAL, Monthly Payment, Note Attach additional sheet if, PLEASE READ THE FOLLOWING BEFORE, Please be advised that your, CERTIFICATION I the undersigned, knowledge, I will apply for any and all, and insurance co real estate co.
Step 3: After you choose the Done button, your ready form can be easily transferred to any of your devices or to email chosen by you.
Step 4: To prevent any sort of risks in the long run, be sure to have as much as several duplicates of your file.
