Filling in uva patient financial services is easy. Our team designed our PDF editor to really make it simple to use and allow you to fill in any form online. Below are a few steps that you should adhere to:
Step 1: Press the orange "Get Form Now" button on the web page.
Step 2: As soon as you've entered the editing page uva patient financial services, you will be able to see every one of the options intended for your form within the upper menu.
Provide the data demanded by the platform to create the document.
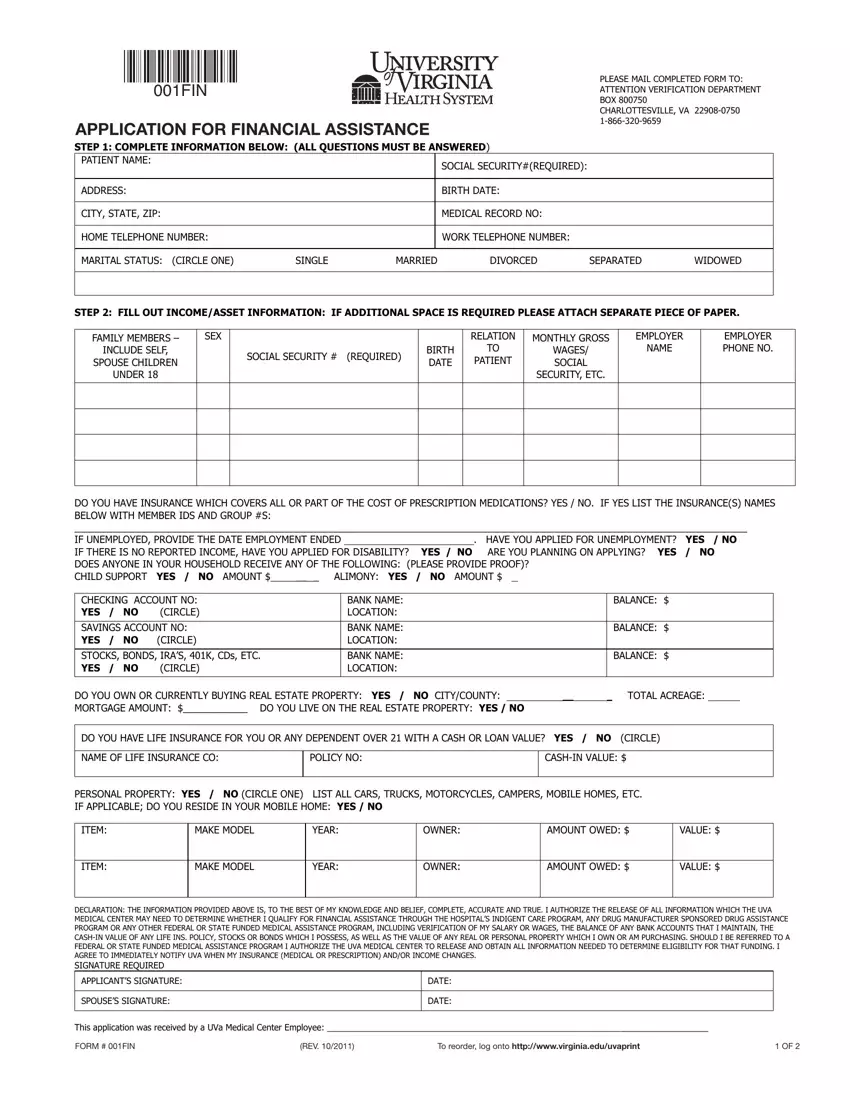
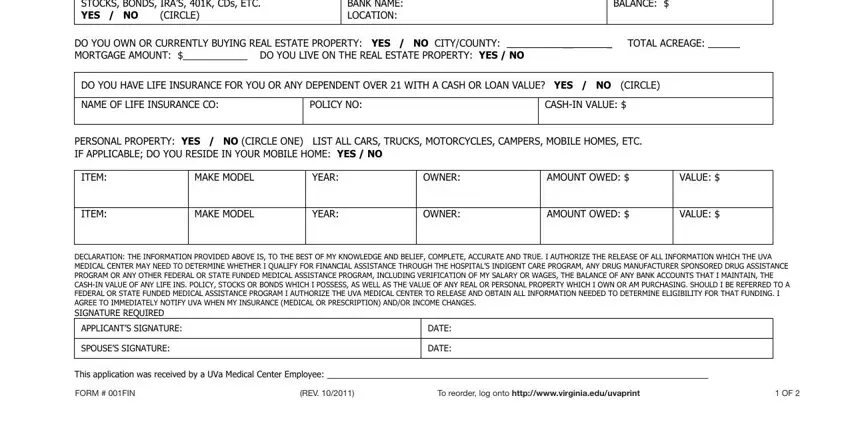
Fill in the STOCKS BONDS IRAS K CDs ETC YES, BANK NAME LOCATION, BALANCE, DO YOU OWN OR CURRENTLY BUYING, TOTAL ACREAGE, DO YOU HAVE LIFE INSURANCE FOR YOU, NAME OF LIFE INSURANCE CO, POLICY NO, CASHIN VALUE, PERSONAL PROPERTY YES NO CIRCLE, ITEM, ITEM, MAKE MODEL, YEAR, and OWNER section with all the particulars requested by the software.
Step 3: If you are done, click the "Done" button to export the PDF document.
Step 4: It is safer to keep copies of the document. You can rest assured that we are not going to reveal or read your details.
