

You can easily get documents working with our PDF editor. Improving the miami home energy assistance program file is simple for those who use these steps:
Step 1: Press the orange "Get Form Now" button on the webpage.
Step 2: The form editing page is now open. It's possible to add information or change existing details.
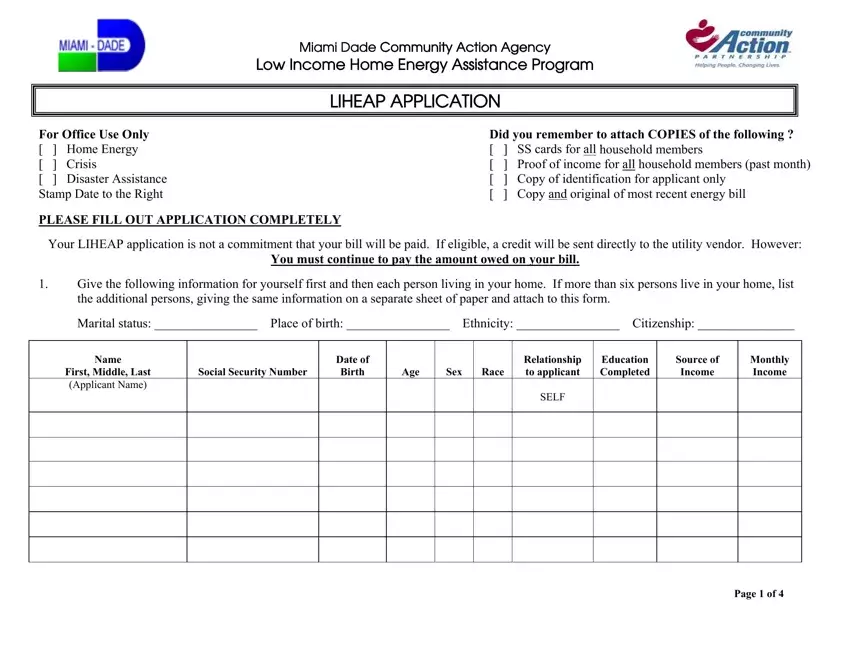
If you want to fill in the miami home energy assistance program PDF, enter the information for each of the parts:
Within the box Page of note the information that the system requires you to do.
You should be requested for certain significant details so you can submit the The address where you are living, Street Number and Name RFD Apt or, FL City or Town Zip Code County, Your mailing address if different, Street Number and Name RFD Apt or, FL City or Town Zip Code County, Day time telephone number where, If your monthly household income, utilities, and Complete the following for your field.
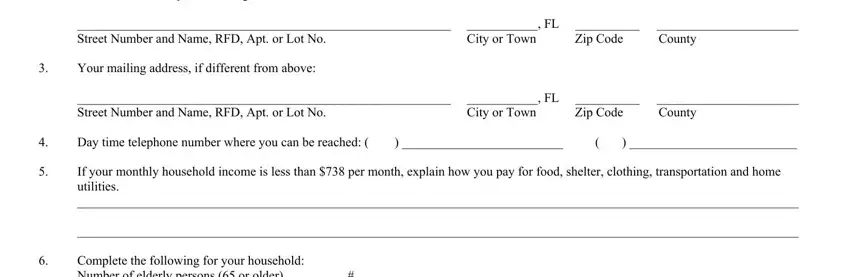
The Complete the following for your, If you share your living or, If you or anyone in your home are, Name Alien Status, and Are you or any member of your field needs to be used to provide the rights or obligations of both sides.
Review the areas Check the programs that anyone in, CSBG, Weatherization, TANFWAGES, Food Stamps, None, If you or any member of your, Name of Agency, Type of help elderly crisis, Date, Do any of the following situations, My electricity has been, I have a shutoff notice from the, I have little or no propone fuel, and If your cost of home energy is and then fill them in.
Step 3: If you're done, select the "Done" button to upload the PDF document.
Step 4: Create copies of your form - it may help you remain away from possible future challenges. And don't be concerned - we do not display or watch your details.
