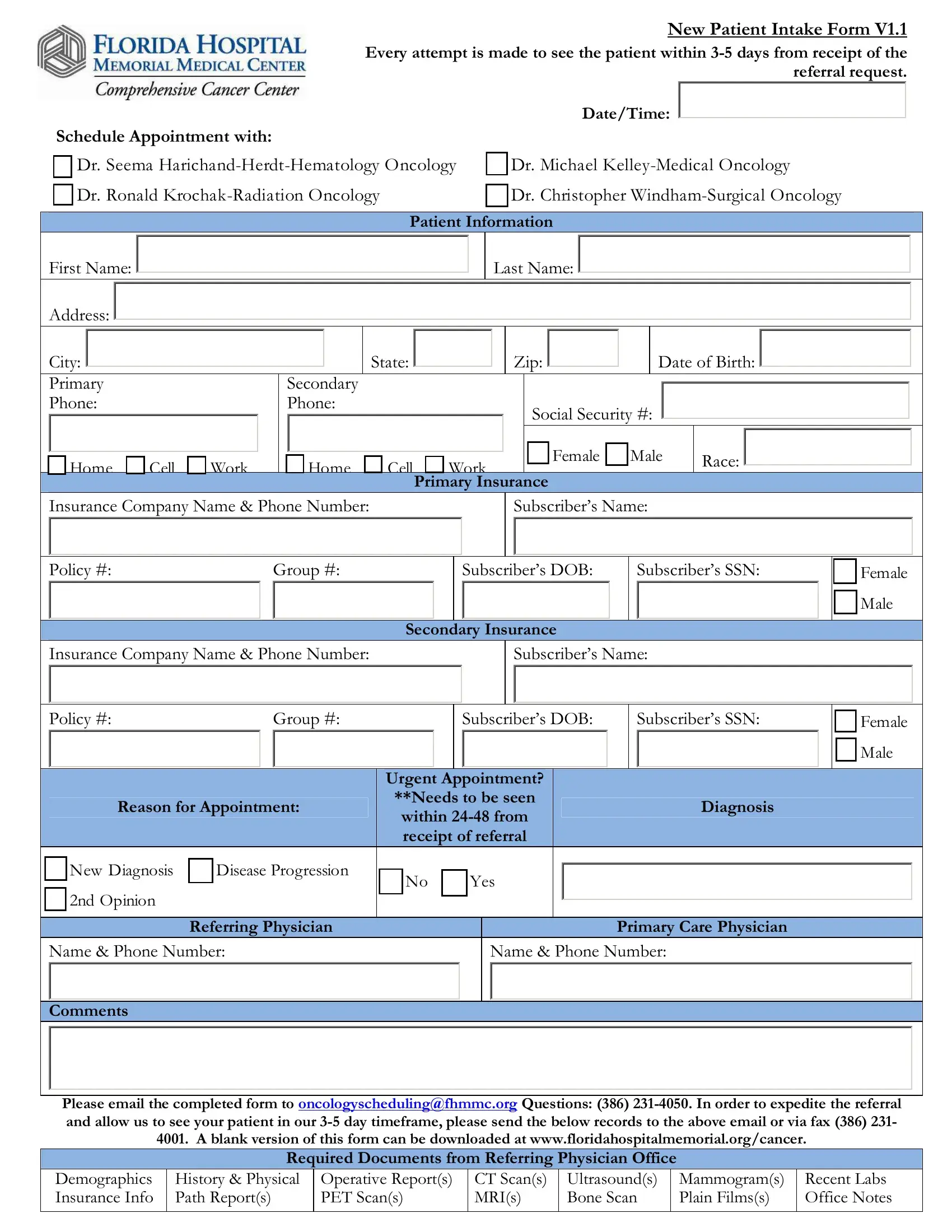
The Florida Hospital form, specifically tailored for new patient intake within their oncology department, epitomizes the intricate blend of administrative efficiency and patient-centered care. It meticulously outlines the crucial steps for scheduling appointments with its specialized oncology team, comprising hematologists, medical and radiation oncologists, and surgical oncologists, ensuring that patients are seen within a stipulated 3-5 day window post-referral. Essential patient information, spanning demographics to detailed insurance data, is systematically collected to facilitate a streamlined care process. Moreover, the form lays out a framework for urgent appointments, diagnoses, and reasons for the appointment, underpinning the hospital's responsive approach to patient needs. Through the mandate of accompanying documents from the referring physician, it underscores the importance of a comprehensive medical history for informed care decisions. The backend processes involving care navigators, the integration with electronic health systems, and protocols for notifying the patient and receiving records form a complex ecosystem aimed at delivering personalized, timely care. This procedural thoroughness not only accelerates the referral process but also emphasizes the hospital's commitment to harnessing detailed patient information and coordination among various specialists to enhance the care trajectory for patients grappling with cancer.
| Question | Answer |
|---|---|
| Form Name | Florida Hospital Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | new form v1 1 pdf, florida hospital discharge papers, hospital discharge papers, hospital intake v1 1 form |