

 I request
I request Creating documents using this PDF editor is simpler as compared to most things. To change friend of the court case questionnaire forms template the form, there isn't anything you need to do - just continue with the actions down below:
Step 1: Select the orange "Get Form Now" button on this page.
Step 2: Now you are going to be within the file edit page. It's possible to add, customize, highlight, check, cross, insert or erase areas or words.
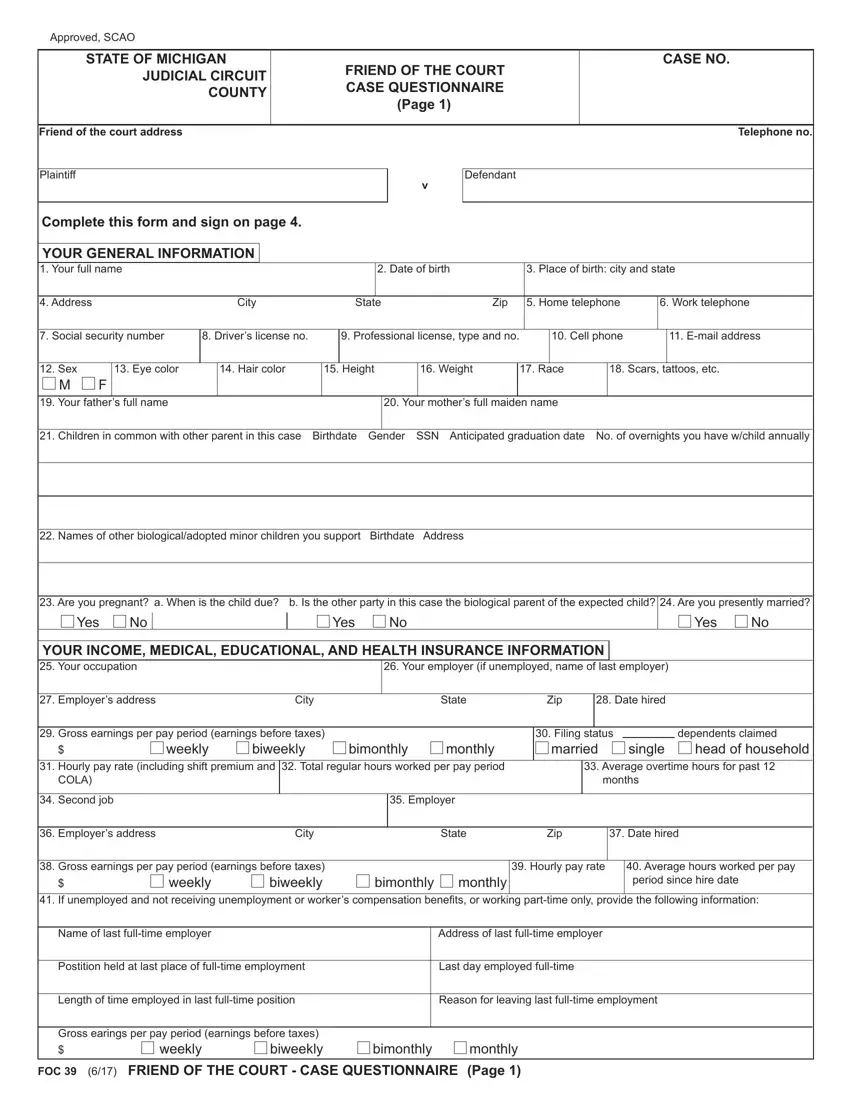
Complete the friend of the court case questionnaire forms template PDF and enter the material for every section:
Fill out the Children in common with other, Names of other biologicaladopted, Are you pregnant a When is the, Yes, Yes, Yes, YOUR INCOME MEDICAL EDUCATIONAL, Your employer if unemployed name, Employers address City State Zip, Date hired, Gross earnings per pay period, Hourly pay rate including shift, biweekly, bimonthly, and monthly areas with any details that is asked by the application.
Write the necessary details in bimonthly If unemployed and not, biweekly, weekly, monthly, Average hours worked per pay, Name of last fulltime employer, Address of last fulltime employer, Postition held at last place of, Last day employed fulltime, Length of time employed in last, Reason for leaving last fulltime, Gross earings per pay period, weekly, biweekly, and bimonthly field.
Please be sure to record the rights and obligations of the parties in the STATE OF MICHIGAN, JUDICIAL CIRCUIT COUNTY, FRIEND OF THE COURT CASE, CASE NO, YOUR INCOME MEDICAL EDUCATIONAL, Commissions, Bonuses, Profit Sharing, Interest, Dividends, Annuities, PensionsLongevity, Deferred CompIRA, Trust Funds, and Unemp Benefits paragraph.
End by analyzing the following sections and completing them accordingly: Do any of the children listed on, Yes, Childs Name, Amount monthly, Type of benefit check one, SSI, Dependent benefit, Source of dependent benefit mother, Attach your four most recent, Yes, What is your educational, less than high school Associates, High school graduate Bachelors, Trade school graduate Graduate, and Medical insurance company name.
Step 3: Select the "Done" button. Next, you can transfer the PDF file - download it to your electronic device or send it by means of email.
Step 4: In order to prevent potential forthcoming problems, ensure that you obtain around two or three duplicates of every single document.
