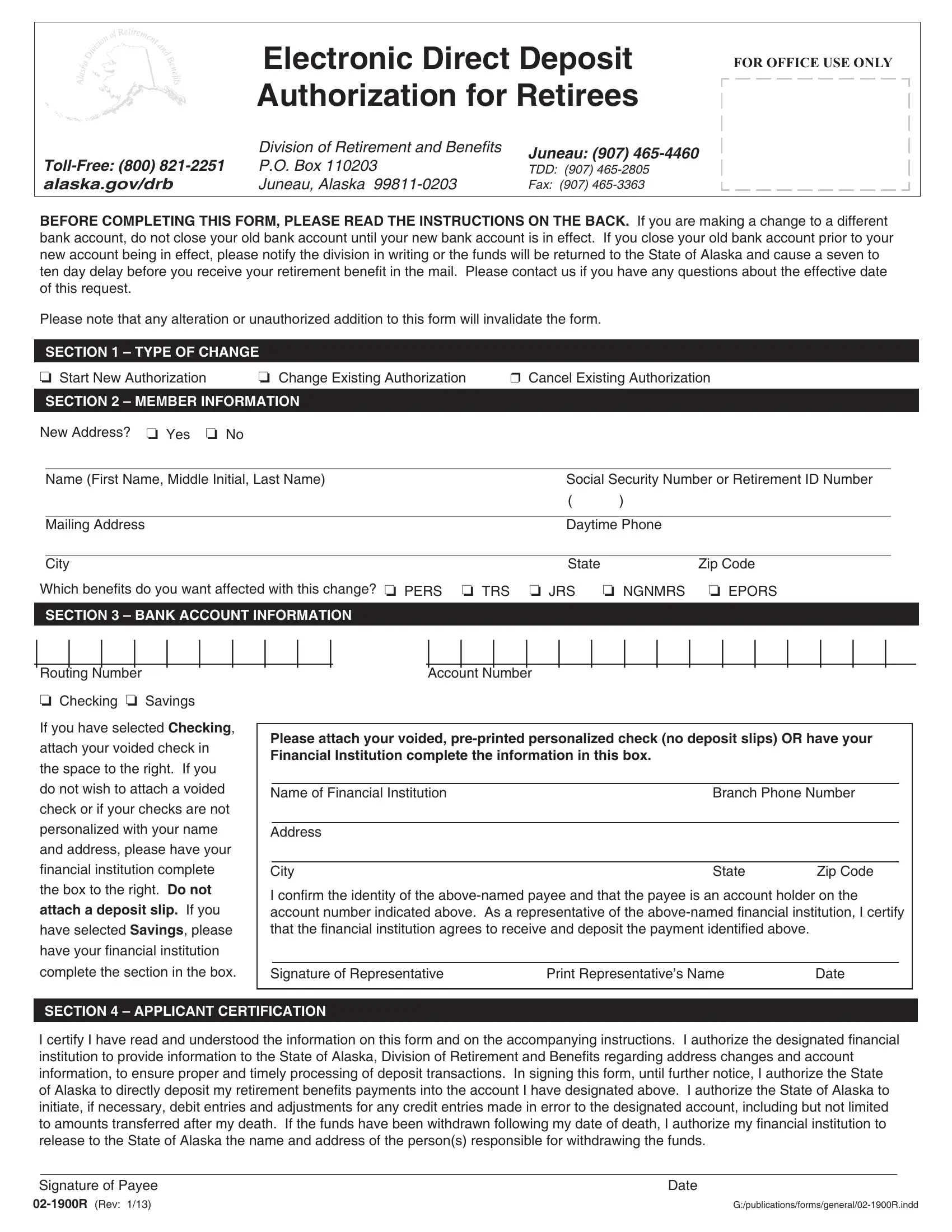
When it comes to managing retirement benefits, ensuring a smooth, secure, and timely transfer of funds is crucial for retirees. The Electronic Direct Deposit Authorization for Retirees form, also known as the 02 1900R form, is designed specifically for this purpose by the Division of Retirement and Benefits in Alaska. Aimed at simplifying the lives of retirees, this form plays a pivotal role in transitioning them from receiving traditional check-based payments to enjoying the benefits of electronic direct deposits. By completing this form, retirees can authorize the direct deposit of their monthly benefits into a designated banking account, whether it be a checking or a savings account. The convenience of electronic deposit not only offers peace of mind by reducing the risk of lost or stolen checks, but it also ensures that retirees have quicker access to their funds. Moreover, the form caters to various updates that retirees might need to make, such as starting a new authorization, changing an existing bank account, or canceling a current direct deposit arrangement. It underscores the importance of keeping a previous account open until the new direct deposit is fully operational, a measure that prevents any interruption in the receipt of benefits. The 02 1900R form also emphasizes the importance of retirees notifying the Division in case of early account closures to avoid delays. Clearly, through meticulous instructions and defined sections for personal and banking information, the form facilitates a smooth transition for retirees, making their post-retirement financial management hassle-free and more secure.
| Question | Answer |
|---|---|
| Form Name | Form 02 1900R |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | 02 1900r suntrust direct deposit form editable |
|
Electronic Direct Deposit |
FOR OFFICE USE ONLY |
|
|
|
||
|
Authorization for Retirees |
|
|
|
Division of Retirement and Beneits |
Juneau: (907) |
|
P.O. BOX 110203 |
|
||
TDD: (907) |
|
||
alaska.gov/drb |
JUNEAU, ALASKA |
FAX: (907) |
|
BEFORE COMPLETING THIS FORM, PLEASE READ THE INSTRUCTIONS ON THE BACK. If you are making a change to a different bank account, do not close your old bank account until your new bank account is in effect. If you close your old bank account prior to your
new account being in effect, please notify the division in writing or the funds will be returned to the State of Alaska and cause a seven to ten day delay before you receive your retirement beneit in the mail. Please contact us if you have any questions about the effective date of this request.
Please note that any alteration or unauthorized addition to this form will invalidate the form.
|
SECTION 1 – TYPE OF CHANGE |
|
|
|
|
❏ Start New Authorization |
❏ Change Existing Authorization |
❒ Cancel Existing Authorization |
|||
|
|
|
|
|
|
|
SECTION 2 – MEMBER INFORMATION |
|
|
|
|
New Address? ❏ Yes ❏ No |
|
|
|
|
|
|
|
|
|
||
|
Name (First Name, Middle Initial, Last Name) |
Social Security Number or Retirement ID Number |
|||
|
|
|
( |
) |
|
|
|
|
|
||
|
Mailing Address |
|
Daytime Phone |
|
|
|
|
|
|
|
|
|
City |
|
State |
Zip Code |
|
Which beneits do you want affected with this change? ❏ PERS ❏ TRS |
❏ JRS |
❏ NGNMRS ❏ EPORS |
|||
|
SECTION 3 – BANK ACCOUNT INFORMATION |
|
|
|
|
|
|
|
|
|
|
| |
| |
| |
| |
| |
| |
| |
|
Routing Number |
|
|
|
||
❏Checking ❏ Savings
If you have selected Checking, attach your voided check in the space to the right. If you do not wish to attach a voided check or if your checks are not personalized with your name and address, please have your
inancial institution complete
the box to the right. Do not
attach a deposit slip. If you
have selected Savings, please
have your inancial institution
complete the section in the box.
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
|
|
|
Account Number |
|
|
|
|
|
|
|
|
|
|
|
|||
Please attach your voided,
Name of Financial Institution |
Branch Phone Number |
|
|
|
|
Address |
|
|
|
|
|
City |
State |
Zip Code |
I conirm the identity of the
Signature of Representative |
Print Representative’s Name |
Date |
SECTION 4 – APPLICANT CERTIFICATION
I certify I have read and understood the information on this form and on the accompanying instructions. I authorize the designated inancial institution to provide information to the State of Alaska, Division of Retirement and Beneits regarding address changes and account
information, to ensure proper and timely processing of deposit transactions. In signing this form, until further notice, I authorize the State
of Alaska to directly deposit my retirement beneits payments into the account I have designated above. I authorize the State of Alaska to
initiate, if necessary, debit entries and adjustments for any credit entries made in error to the designated account, including but not limited
to amounts transferred after my death. If the funds have been withdrawn following my date of death, I authorize my inancial institution to
release to the State of Alaska the name and address of the person(s) responsible for withdrawing the funds.
Signature of Payee |
Date |
Alaska Division of Retirement and Beneits
Electronic Direct Deposit Instructions
The State of Alaska, Division of Retirement and Beneits (DRB) is pleased to offer you the convenience of electronic deposit of your monthly retirement beneit. Please follow these instructions to complete your Direct Deposit Request. This offer to participate in electronic direct
deposit complies with AS 37.25.050 and 2 AAC 15.130. By submitting this form you are authorizing the DRB to transmit any retirement beneits due by electronic funds transfer to the designated account.
If at any time the amount of beneits deposited exceeds the amount of beneits actually due and payable to you, you hereby authorize DRB to either:
(1)Withhold a sum equal to the overpayment from future beneits; or
(2)Recover such overpayment from the
This authorization remains in full force and effect until we receive written notiication from you of its termination or when beneits are no longer payable.
INSTRUCTIONS
Section 1 – Check the appropriate box to indicate the type of authorization you are requesting.
•Choose Start New Authorization if you are a new retiree or have not previously set up a direct deposit account for your monthly beneit.
•Choose Change Existing Authorization if you would like to change the account number and/or inancial institution of an existing account. Do not close your old account until your irst payment is deposited into your newly designated account and/or inancial institution.
•Choose Cancel Existing Authorization if you would like to cancel your current direct deposit and receive your check through the U.S. Mail.
Section 2 – Member Information
•Please check whether or not the address you are writing on this document is new.
•Print your First Name, Middle Initial, and Last Name, as well as your Social Security Number or Retirement Identiication Number (RIN).
•Print your Mailing Address, City, State and Zip Code, as well as a Daytime Phone Number.
•Multiple Retirement Beneits Information – Indicate which retirement beneit(s) you want affected by this change. If you are unsure how to complete this section, please contact the Retiree Payroll Section at the numbers listed at the top of the form.
Section 3 – Bank Account Information
•Enter the Routing Number and the Account Number.
•Indicate whether you wish to have funds deposited into either your checking or savings account. Select only one.
•If you select Checking, attach a voided,
•If you select Savings, you will need to bring the form to your inancial institution and have them complete the Financial Institution information in the box.
Note: Your inancial institution must be a member of the Automated Clearing House Association to accept a direct deposit from DRB. DRB cannot make direct deposits to a bank or inancial institution outside of the United States.
Section 4 – Applicant Certiication
•Sign your legal name as the authorizing payee or authorized legal representative. Date the form with the current date. All requested
information must be completed and form must be signed to initiate an electronic deposit. Items left blank will delay processing the transfer of funds. Authorized legal representatives must have appropriate documentation on ile with DRB.
Submitting the form
•You may fax the form to the fax number listed at the top of the form.
•You may scan and then email the form to doa.drb.payroll@alaska.gov.
•You may mail the form to the address listed at the top of the form, attention “Retiree Payroll Section.”