

Through the online tool for PDF editing by FormsPal, you're able to complete or modify DDS-1 here and now. We are devoted to making sure you have the perfect experience with our tool by constantly adding new features and enhancements. With these improvements, working with our editor gets better than ever before! Getting underway is simple! All that you should do is stick to the following easy steps directly below:
Step 1: Just press the "Get Form Button" at the top of this site to access our form editor. There you will find everything that is required to fill out your document.
Step 2: As you access the PDF editor, you will get the document ready to be filled in. Apart from filling in various blanks, you may as well do some other actions with the PDF, specifically putting on custom text, editing the initial textual content, adding images, affixing your signature to the PDF, and more.
This PDF form will need specific information to be filled in, thus ensure you take whatever time to fill in precisely what is requested:
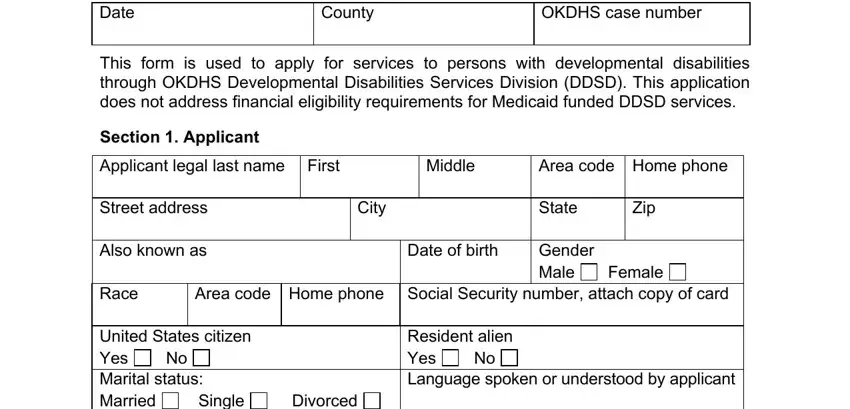
1. It is critical to complete the DDS-1 properly, therefore be attentive while filling out the areas containing all these blank fields:
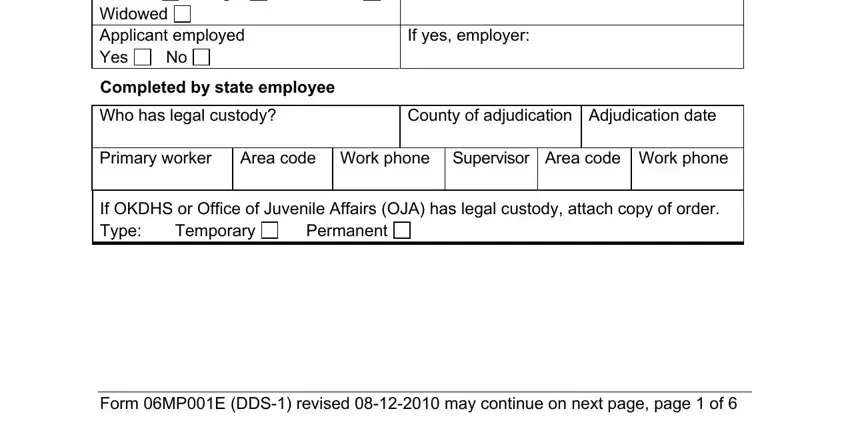
2. Soon after filling in this step, go on to the subsequent part and complete all required details in these blanks - United States citizen Yes Marital, Single, Divorced, If yes employer, Completed by state employee, Who has legal custody, County of adjudication, Primary worker Area code Work, If OKDHS or Office of Juvenile, Permanent, Temporary, and Form MPE DDS revised may continue.
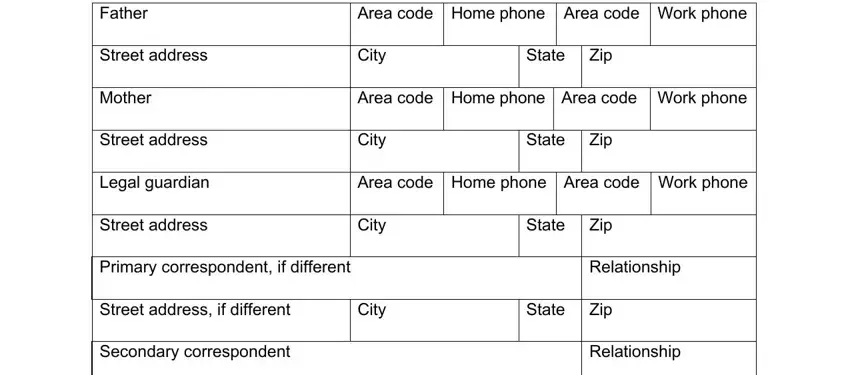
3. The following portion is all about Father, Area code Home phone Area code, Street address, City, State Zip, Mother, Area code Home phone Area code, Street address, City, State Zip, Legal guardian, Area code Home phone Area code, Street address, City, and State Zip - fill in each one of these fields.
4. The fourth paragraph arrives with all of the following blank fields to type in your details in: Street address, City, State Zip, Section Household members, Name, Relationship, Date of, birth, Occupation, and Health status.
5. The document must be finalized by going through this section. Further you can find a comprehensive list of form fields that require correct details to allow your document submission to be complete: Section Medical, Attach copy of applicants birth, and Form MPE DDS revised may continue.
Always be really attentive while filling in Section Medical and Attach copy of applicants birth, as this is the part in which most users make mistakes.
Step 3: Before submitting this file, it's a good idea to ensure that blank fields have been filled in the correct way. As soon as you are satisfied with it, press “Done." Make a free trial subscription at FormsPal and gain immediate access to DDS-1 - download or edit in your personal cabinet. FormsPal guarantees your data privacy by using a protected method that never saves or shares any private data involved. Feel safe knowing your docs are kept confidential each time you work with our services!