In an era where the cost of healthcare continues to be a paramount concern for many, programs like the VELCADE Reimbursement Assistance Program come as a beacon of hope, especially for those needing critical medication but facing financial hurdles. Established by Millennium Pharmaceuticals, Inc., this program transcends mere corporate responsibility; it offers a lifeline by facilitating the process of insurance verification and assessing eligibility for assistance with VELCADETM (bortezomib) for Injection, a significant therapeutic option for certain conditions. Eligibility criteria are meticulously set to encompass healthcare providers, patients, and caregivers, ensuring a wide net of support. The comprehensive form required for enrollment is not only a testament to the detailed process designed to verify health insurance coverage and ascertain any co-pay obligations but also a medium through which preauthorization and drug coverage assessments are streamlined. The inclusion of sections dedicated to both the patient and prescribing physician underscores a collaborative approach towards patient care, requesting detailed information that ensures a holistic understanding of the patient's financial and medical background. The submission process, requiring the form to be faxed or mailed, although seemingly traditional, underscores the importance of a tangible review in the determination of eligibility and assistance levels. With sections devoted to financial information and explicit consent for sharing personal health information, the form intricately balances the need for comprehensive data collection with the imperative of maintaining patient confidentiality and autonomy in the healthcare discourse.
| Question | Answer |
|---|---|
| Form Name | Form 1 866 Velcade |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | 2003, VELCADETM, insurer, W-2 |
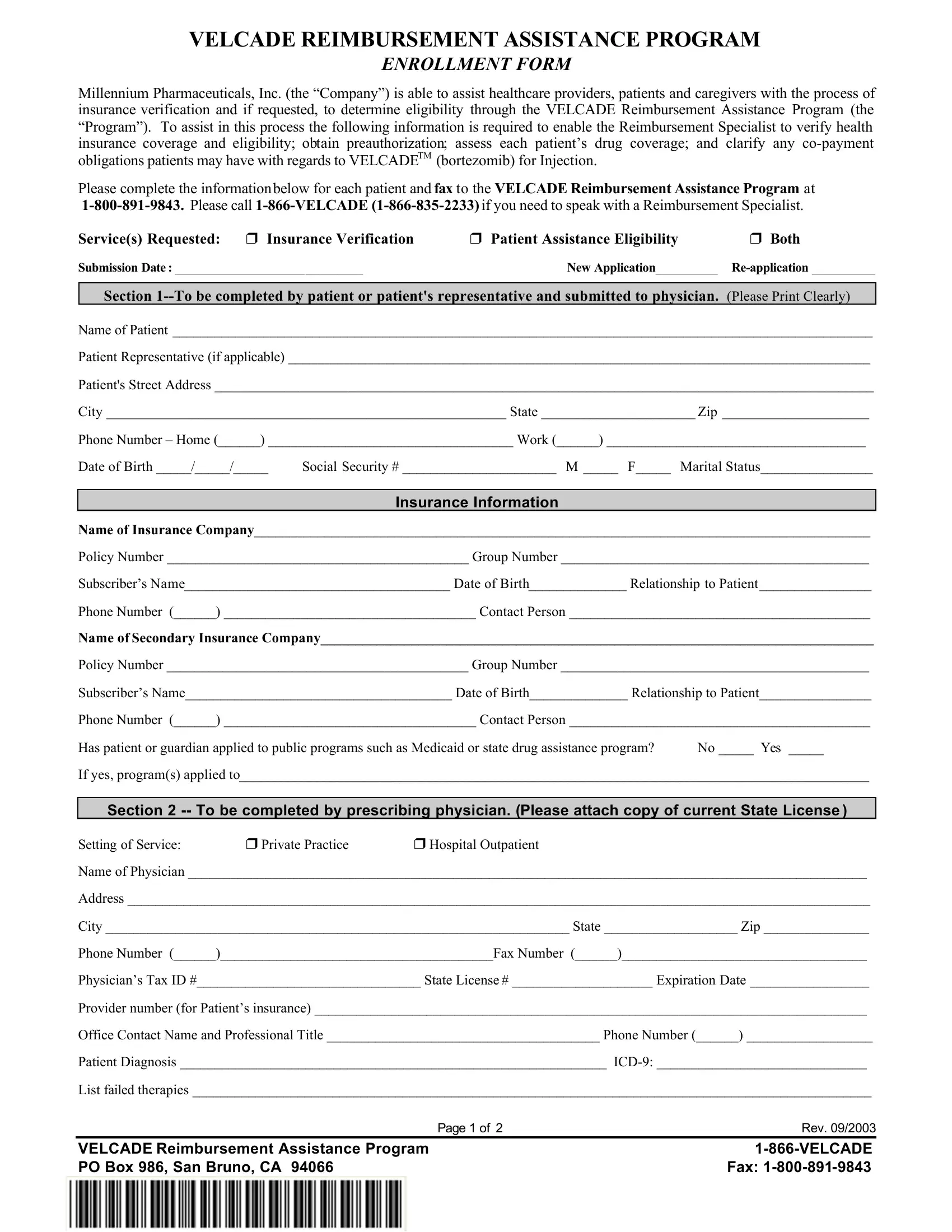
VELCADE REIMBURSEMENT ASSISTANCE PROGRAM
ENROLLMENT FORM
Millennium Pharmaceuticals, Inc. (the “Company”) is able to assist healthcare providers, patients and caregivers with the process of insurance verification and if requested, to determine eligibility through the VELCADE Reimbursement Assistance Program (the “Program”). To assist in this process the following information is required to enable the Reimbursement Specialist to verify health insurance coverage and eligibility; obtain preauthorization; assess each patient’s drug coverage; and clarify any
Please complete the informationbelow for each patient and fax to the VELCADE Reimbursement Assistance Program at
Service(s) Requested: |
r Insurance Verification |
r Patient Assistance Eligibility |
r Both |
Submission Date: ______________________________ |
New Application__________ |
||
Section
Name of Patient ____________________________________________________________________________________________________
Patient Representative (if applicable) ___________________________________________________________________________________
Patient's Street Address ______________________________________________________________________________________________
City _________________________________________________________ State ______________________ Zip _____________________
Phone Number – Home (______) ___________________________________ Work (______) _____________________________________
Date of Birth _____/_____/_____ Social Security # ______________________ M _____ F_____ Marital Status________________
Insurance Information
Name of Insurance Company________________________________________________________________________________________
Policy Number ___________________________________________ Group Number ____________________________________________
Subscriber’s Name______________________________________ Date of Birth______________ Relationship to Patient________________
Phone Number (______) ____________________________________ Contact Person ___________________________________________
Name of Secondary Insurance Company_______________________________________________________________________________
Policy Number ___________________________________________ Group Number ____________________________________________
Subscriber’s Name______________________________________ Date of Birth______________ Relationship to Patient________________
Phone Number (______) ____________________________________ Contact Person ___________________________________________
Has patient or guardian applied to public programs such as Medicaid or state drug assistance program? No _____ Yes _____
If yes, program(s) applied to__________________________________________________________________________________________
Section 2
Setting of Service: r Private Practice r Hospital Outpatient
Name of Physician _________________________________________________________________________________________________
Address __________________________________________________________________________________________________________
City __________________________________________________________________ State ___________________ Zip _______________
Phone Number (______)_______________________________________Fax Number (______)___________________________________
Physician’s Tax ID #________________________________ State License # ____________________ Expiration Date _________________
Provider number (for Patient’s insurance) _______________________________________________________________________________
Office Contact Name and Professional Title _______________________________________ Phone Number (______) __________________
Patient Diagnosis _____________________________________________________________
List failed therapies _________________________________________________________________________________________________
Page 1 of 2 |
Rev. 09/2003 |
VELCADE Reimbursement Assistance Program |
|
PO Box 986, San Bruno, CA 94066 |
Fax: |
If eligibility for patient assistance is established, the completed original form with signature must be faxed or mailed to the address below.
VELCADE Reimbursement Assistance Program
MILLENNIUM Pharmaceuticals, Inc.
P.O. Box 986, San Bruno, CA 94066
Fax
Toll Free #
Financial Information |
|
Financial Information- Only if applying for Patient Assistance |
|
Annual Household Income |
_________________________ |
(Include Salary/Wages, Pension, Social Security, SSI, SS Disability, Unemployment) |
|
Number of People in Household |
_________________________ |
Proof of Income is required before any drug is distributed.
Please attach a copy of most recent federal tax return or
Applicant Declaration
Financial Statement:
I certify that the information provided in this form is correct and complete. If needed, Millennium Pharmaceuticals, Inc. (“the Company”) and the patient assistance program (“the Program”) may request and obtain information about my, or my family’s income to enroll me in the Program. I understand that my information will be verified every 6 months and that I will need to reapply to this Program everytwelve months.
Permission for Sharing Personal Health Information:
To confirm that I qualify for the Program, my doctor may give a representative of the Program information about my health. My insurer and employer may give the Program information about my insurance. People who work for and with the Company to run the Program may see my health and insurance information and the information on this form, but they may use it only for this Program. The Program will make every effort to keep my information confidential, but if it is accidentally disclosed, federal privacy laws will not protect it.
This permission will last for one year from the time I apply to the Program. If I change my mind before one year has passed, I can call the Program’s
I understand that I may refuse to sign this form and that doing so will not affect my doctor’s treatment of me or my eligibility for insurance benefits.
X
Signature of Patient or Patient Representative (if signed by Representative, explain authority to act for the Patient)
Name |
Date |
Physician Declaration
To the best of my knowledge, this patient does not have any prescription drug coverage (includingprivate insurance, Medicare, Medicaid, county funded assistance, or other public programs) for VELCADE™ (bortezomib) for Injection.
No claim may be made to any third party payer for payment of product provided under the Program. Product provided under the Program must only be used for the approved patient and may not be sold, traded or returned for credit. The VELCADE Reimbursement Assistance Program requests that physicians do not charge the patient for those professional services associated with this regimen that are not covered by the patient’s health insurer.
Please indicate that you agree to these terms by signing below. Failure to comply with these terms may mean you (and any patients you treat) will no longer be eligible to participate in the VELCADEReimbursement Assistance Program. Your signature confirms that there is a valid medical need for this patient’s prescription.
Physician Signature : ___________________________________________________________________________________________________________
Physician Name (Print): _________________________________________________________ |
Date: _________________________________________ |
Page 2 of 2 |
Rev. 09/2003 |
VELCADE Reimbursement Assistance Program |
|
PO Box 986, San Bruno, CA 94066 |
Fax: |