Navigating the landscape of obtaining or releasing confidential information within the framework of the Agency for Persons with Disabilities involves understanding and utilizing the 10-003 form accurately. This document serves as a versatile tool, offering individuals the ability to consent to either obtain protected health information or allow its release to specified entities. It covers a broad spectrum of information types including medical, social service, academic, and various therapeutic reports, among others. Designed to safeguard the privacy and control individuals have over their personal information, the form requires explicit permission for the agency or its representatives to fetch or disclose information. Additionally, it outlines the rights of the consenting individual, emphasizing the importance of informed consent and the conditions under which information may be re-released. The procedural aspect of this form, including the necessity of a legal representative in certain cases, the option to revoke consent, and the specific validity period of the authorization, highlights the meticulous considerations taken to protect individuals' rights. Whether for obtaining necessary services or coordinating care among multiple providers, the 10-003 form plays a crucial role in facilitating the exchange of essential health information while maintaining compliance with privacy regulations.
| Question | Answer |
|---|---|
| Form Name | Form 10 003 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | form apd persons release information, form apd release information online, apd persons release information form, form apd release form |
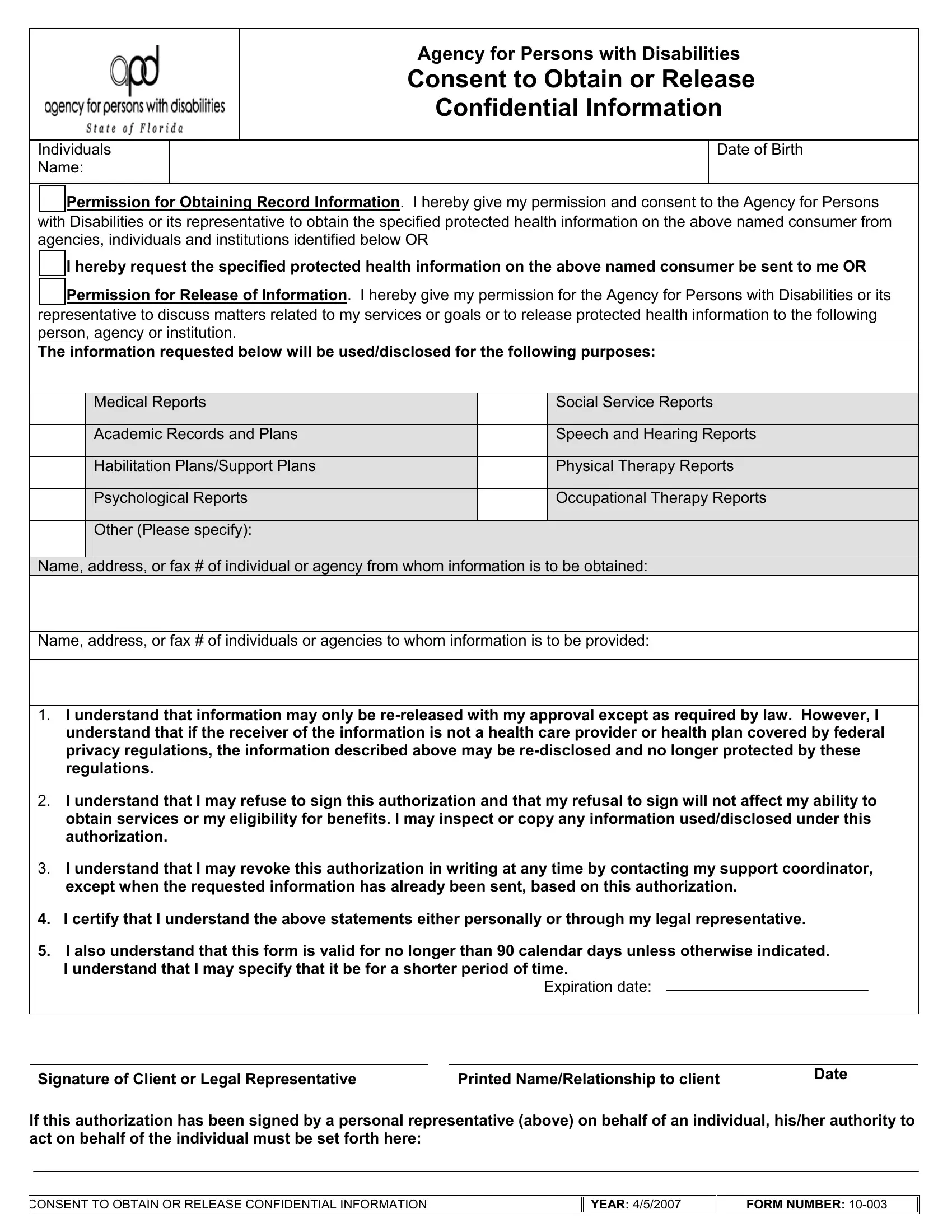
Individuals Name:
Agency for Persons with Disabilities
Consent to Obtain or Release Confidential Information
Date of Birth
Permission for Obtaining Record Information. I hereby give my permission and consent to the Agency for Persons with Disabilities or its representative to obtain the specified protected health information on the above named consumer from agencies, individuals and institutions identified below OR
I hereby request the specified protected health information on the above named consumer be sent to me OR
Permission for Release of Information. I hereby give my permission for the Agency for Persons with Disabilities or its representative to discuss matters related to my services or goals or to release protected health information to the following person, agency or institution.
The information requested below will be used/disclosed for the following purposes:
|
Medical Reports |
|
Social Service Reports |
|
|
|
|
|
Academic Records and Plans |
|
Speech and Hearing Reports |
|
|
|
|
|
Habilitation Plans/Support Plans |
|
Physical Therapy Reports |
|
|
|
|
|
Psychological Reports |
|
Occupational Therapy Reports |
|
|
|
|
|
Other (Please specify): |
|
|
|
|
|
|
Name, address, or fax # of individual or agency from whom information is to be obtained:
Name, address, or fax # of individuals or agencies to whom information is to be provided:
1.I understand that information may only be
2.I understand that I may refuse to sign this authorization and that my refusal to sign will not affect my ability to obtain services or my eligibility for benefits. I may inspect or copy any information used/disclosed under this authorization.
3.I understand that I may revoke this authorization in writing at any time by contacting my support coordinator, except when the requested information has already been sent, based on this authorization.
4.I certify that I understand the above statements either personally or through my legal representative.
5.I also understand that this form is valid for no longer than 90 calendar days unless otherwise indicated.
I understand that I may specify that it be for a shorter period of time.
Expiration date:
Signature of Client or Legal Representative |
Printed Name/Relationship to client |
Date |
|
If this authorization has been signed by a personal representative (above) on behalf of an individual, his/her authority to act on behalf of the individual must be set forth here:
CONSENT TO OBTAIN OR RELEASE CONFIDENTIAL INFORMATION |
YEAR: 4/5/2007 |
FORM NUMBER: