


When you want to fill out PREPARER, it's not necessary to download and install any applications - simply give a try to our PDF tool. To have our editor on the forefront of efficiency, we strive to put into practice user-oriented capabilities and enhancements regularly. We're at all times glad to receive suggestions - play a pivotal part in reshaping PDF editing. If you're seeking to get started, this is what it requires:
Step 1: Simply click on the "Get Form Button" above on this page to get into our pdf form editing tool. Here you will find everything that is necessary to fill out your document.
Step 2: The editor offers the capability to work with your PDF in various ways. Modify it by adding your own text, correct what's originally in the document, and add a signature - all when it's needed!
Completing this document will require attention to detail. Make certain every field is filled out properly.
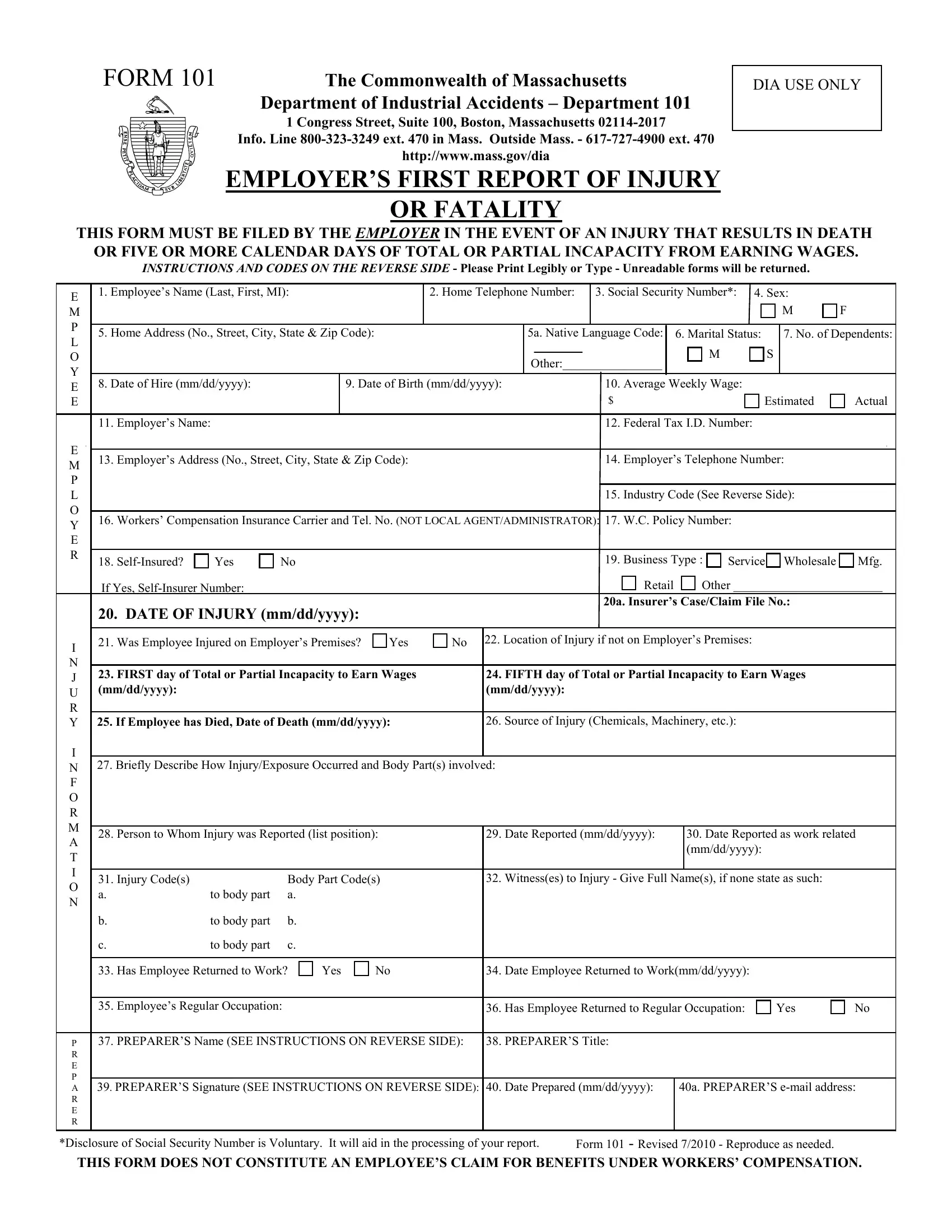
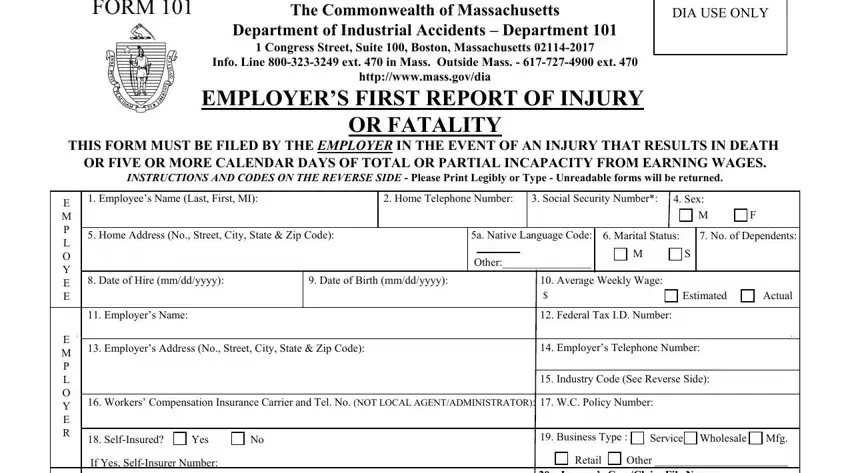
1. While filling in the PREPARER, ensure to incorporate all of the necessary blank fields in its relevant area. This will help expedite the process, which allows your details to be processed without delay and correctly.
2. Once your current task is complete, take the next step – fill out all of these fields - DATE OF INJURY mmddyyyy, a Insurers CaseClaim File No, Was Employee Injured on Employers, Location of Injury if not on, FIRST day of Total or Partial, FIFTH day of Total or Partial, If Employee has Died Date of, Source of Injury Chemicals, Briefly Describe How, Person to Whom Injury was, Date Reported mmddyyyy, Date Reported as work related, Injury Codes a, to body part, and Body Part Codes a with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
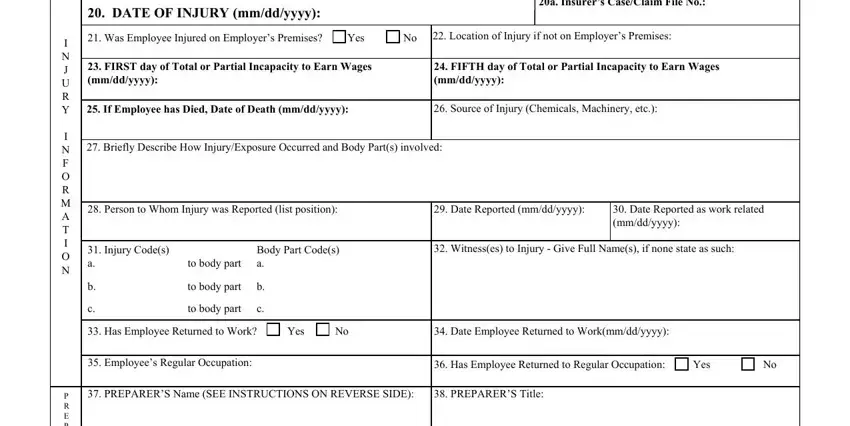
Always be extremely attentive when completing If Employee has Died Date of and to body part, because this is the part where a lot of people make a few mistakes.
3. In this step, review PREPARERS Signature SEE, a PREPARERS email address, P R E P A R E R, Disclosure of Social Security, Form Revised Reproduce as, and THIS FORM DOES NOT CONSTITUTE AN. Each one of these need to be filled in with greatest precision.

Step 3: Just after rereading your fields and details, hit "Done" and you're good to go! Right after creating a7-day free trial account here, you'll be able to download PREPARER or email it without delay. The file will also be available via your personal account page with your adjustments. FormsPal is devoted to the privacy of all our users; we ensure that all information entered into our system is kept secure.