It is simple to fill out forms using our PDF editor. Editing the human appeals form document is effortless as soon as you keep to these actions:
Step 1: Pick the button "Get Form Here".
Step 2: Once you have accessed the human appeals form edit page, you'll discover all options you may undertake concerning your document at the top menu.
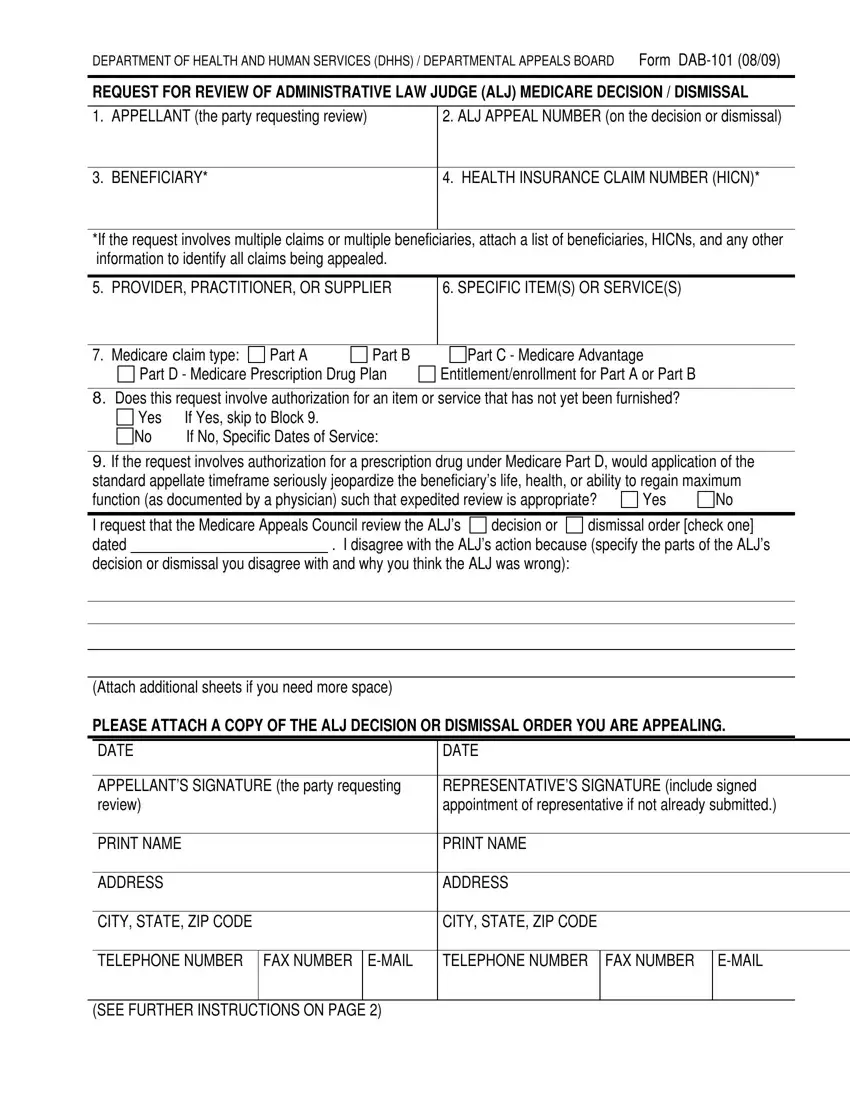
Prepare the human appeals form PDF by providing the details required for every single area.
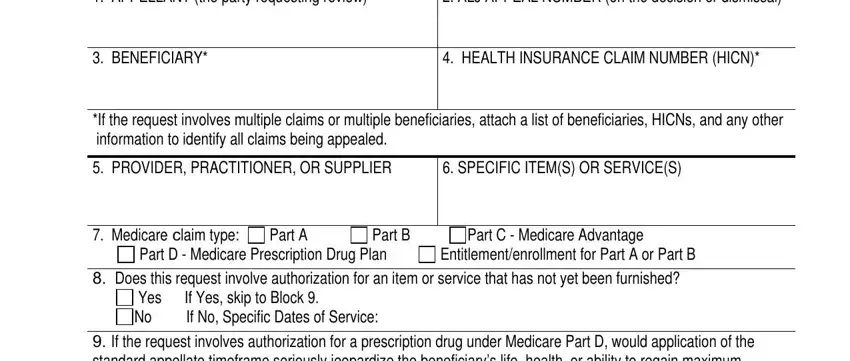
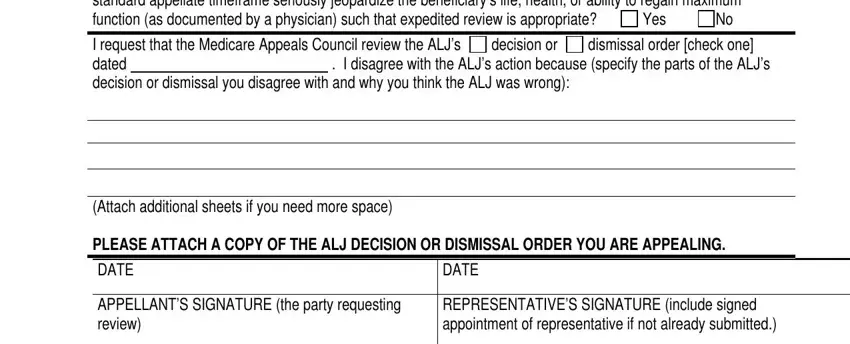
Inside the field Yes If Yes skip to Block No If No, I request that the Medicare, dismissal order check one, decision or, Attach additional sheets if you, PLEASE ATTACH A COPY OF THE ALJ, DATE, DATE, APPELLANTS SIGNATURE the party, and REPRESENTATIVES SIGNATURE include enter the information that the system requires you to do.
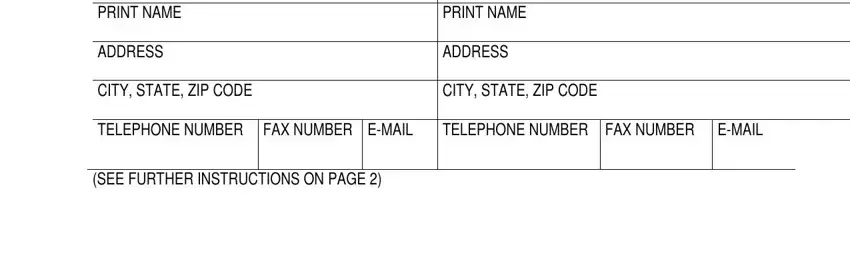
The application will require for further details with a purpose to easily fill in the box PRINT NAME, ADDRESS, PRINT NAME, ADDRESS, CITY STATE ZIP CODE, CITY STATE ZIP CODE, TELEPHONE NUMBER, FAX NUMBER EMAIL, TELEPHONE NUMBER FAX NUMBER, EMAIL, and SEE FURTHER INSTRUCTIONS ON PAGE.
The space If you are a provider supplier or, IMPORTANT Include the HICN and ALJ, This request must be received, You must file your request for, Department of Health and Human, and You may send the request for is going to be where you can insert both sides' rights and responsibilities.
End by reviewing these areas and filling them in accordingly: If you have any questions about, PRIVACY ACT STATEMENT, and The collection of information on.
Step 3: Press "Done". Now you may export your PDF document.
Step 4: Get duplicates of the file. This is going to save you from upcoming difficulties. We cannot look at or reveal your data, thus be assured it is protected.
