
It is possible to prepare form 1199a june easily in our PDF editor online. Our tool is constantly developing to present the best user experience achievable, and that's due to our resolve for continuous improvement and listening closely to user comments. It merely requires just a few easy steps:
Step 1: Click on the "Get Form" button above on this page to get into our editor.
Step 2: With this state-of-the-art PDF editor, it is possible to accomplish more than simply complete blanks. Express yourself and make your docs appear professional with custom textual content put in, or tweak the original input to excellence - all that accompanied by the capability to insert just about any images and sign the file off.
This PDF doc will involve specific details; to ensure consistency, be sure to bear in mind the following recommendations:
1. While submitting the form 1199a june, be certain to include all of the essential blank fields within its associated area. It will help to hasten the process, allowing your details to be handled quickly and appropriately.
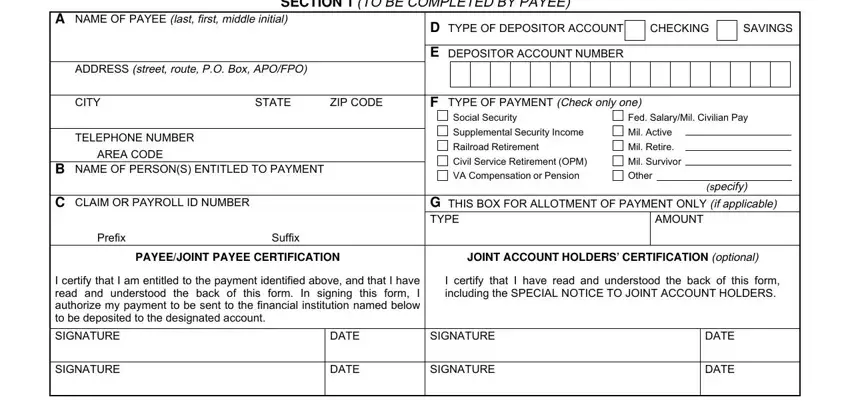
2. Soon after filling out the previous part, head on to the next step and enter the essential details in all these blank fields - GOVERNMENT AGENCY NAME, GOVERNMENT AGENCY ADDRESS, SECTION TO BE COMPLETED BY PAYEE, NAME AND ADDRESS OF FINANCIAL, SECTION TO BE COMPLETED BY, ROUTING NUMBER, DEPOSITOR ACCOUNT TITLE, CHECK DIGIT, I confirm the identity of the, PRINT OR TYPE REPRESENTATIVES NAME, SIGNATURE OF REPRESENTATIVE, TELEPHONE NUMBER, DATE, FINANCIAL INSTITUTION CERTIFICATION, and THE FINANCIAL INSTITUTION SHOULD.
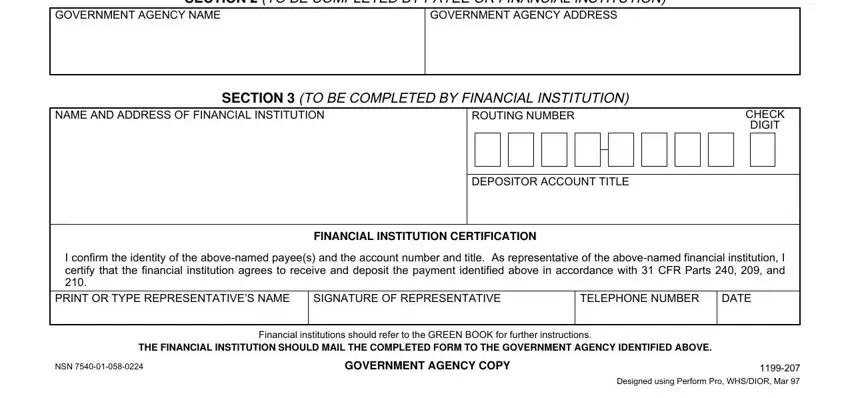
Many people often make mistakes while filling in DATE in this area. You should definitely read again everything you type in right here.
Step 3: Proofread all the information you have entered into the form fields and click on the "Done" button. Join FormsPal today and instantly use form 1199a june, set for downloading. Each change you make is conveniently preserved , so that you can change the pdf later on as needed. At FormsPal, we endeavor to guarantee that your information is kept secure.