If you're like most people, at some point you've probably had to deal with the Internal Revenue Service (IRS). And if you're like most people, you may not have been too thrilled about it. One of the many forms that the IRS requires Americans to fill out is Form 1402. This form is used to report interest and dividends that you've earned during the tax year. While it may seem confusing at first, don't worry – we're here to help! In this blog post, we'll explain what Form 1402 is, and we'll give you a step-by-step guide on how to complete it. So whether you're a first-time tax filer or you just need a refresher course, keep reading for everything you need to know about Form 1402.
| Question | Answer |
|---|---|
| Form Name | Form 1402 Ok |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | 2005, OSDH, dba, 1st |
D&S DIVERSIFIED TECHNOLOGIES LLP dba HEADMASTER LLP
PO BOX 6609 HELENA MT 59604
TELEPHONE:
EMAIL: hdmaster@hdmaster.com
WEB SITE: www.hdmaster.com
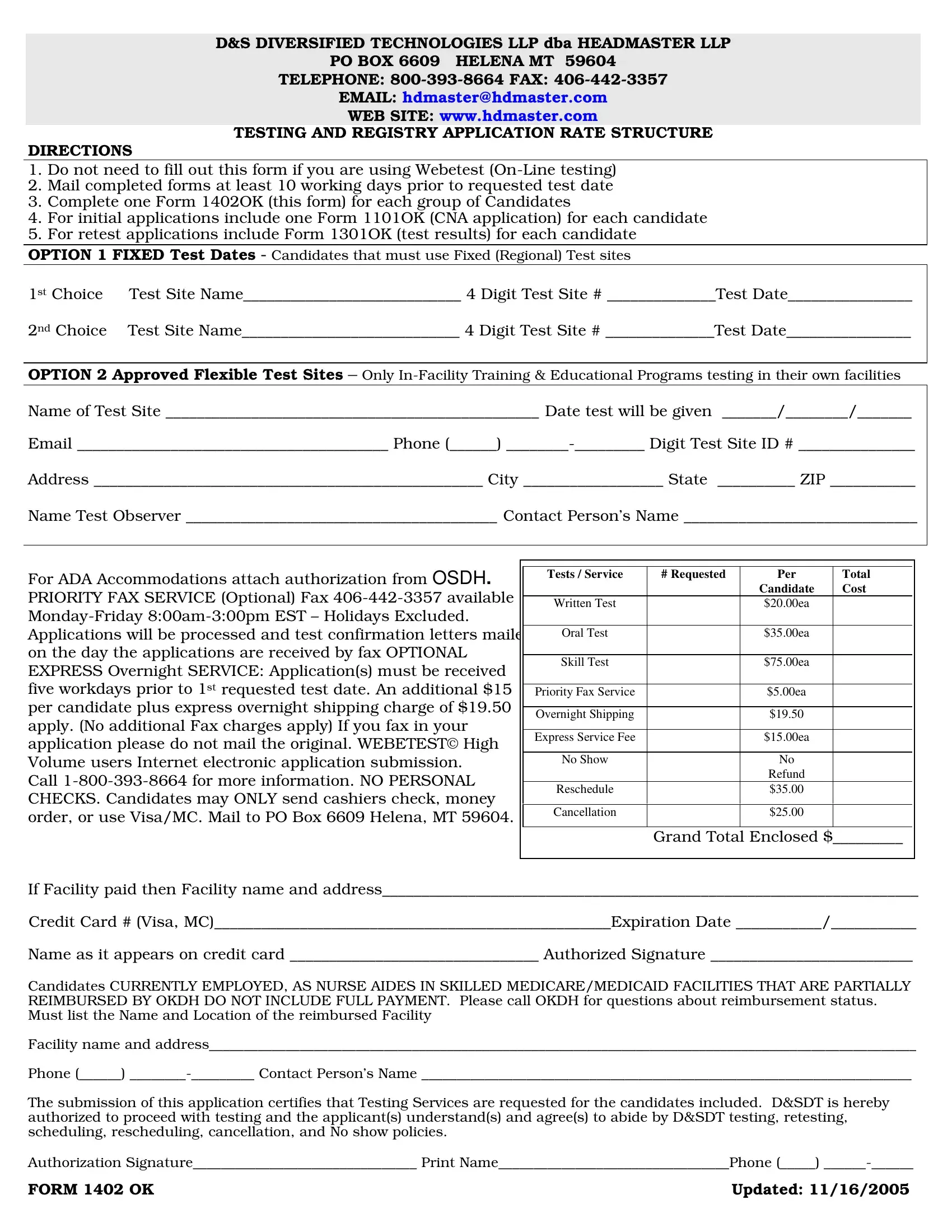
TESTING AND REGISTRY APPLICATION RATE STRUCTURE
DIRECTIONS
1.Do not need to fill out this form if you are using Webetest
2.Mail completed forms at least 10 working days prior to requested test date
3.Complete one Form 1402OK (this form) for each group of Candidates
4.For initial applications include one Form 1101OK (CNA application) for each candidate
5.For retest applications include Form 1301OK (test results) for each candidate
OPTION 1 FIXED Test Dates - Candidates that must use Fixed (Regional) Test sites
1st Choice |
Test Site Name____________________________ 4 Digit Test Site # ______________Test Date________________ |
2nd Choice |
Test Site Name____________________________ 4 Digit Test Site # ______________Test Date________________ |
OPTION 2 Approved Flexible Test Sites – Only
Name of Test Site ________________________________________________ Date test will be given _______/________/_______
Email ________________________________________ Phone (______)
Address __________________________________________________ City __________________ State __________ ZIP ___________
Name Test Observer ________________________________________ Contact Person’s Name ______________________________
|
|
|
|
|
|
|
|
For ADA Accommodations attach authorization from OSDH. |
|
|
Tests / Service |
# Requested |
Per |
Total |
|
|
|
|
|
Candidate |
Cost |
||
PRIORITY FAX SERVICE (Optional) Fax |
|
|
|
|
|||
|
|
Written Test |
|
$20.00ea |
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
Applications will be processed and test confirmation letters mailed |
|
|
Oral Test |
|
$35.00ea |
|
|
on the day the applications are received by fax OPTIONAL |
|
|
|
|
|
|
|
|
|
Skill Test |
|
$75.00ea |
|
|
|
EXPRESS Overnight SERVICE: Application(s) must be received |
|
|
|
|
|
||
|
|
|
|
|
|
|
|
five workdays prior to 1st requested test date. An additional $15 |
|
|
|
|
|
|
|
|
|
Priority Fax Service |
|
$5.00ea |
|
|
|
per candidate plus express overnight shipping charge of $19.50 |
|
|
|
|
|
|
|
|
|
Overnight Shipping |
|
$19.50 |
|
|
|
apply. (No additional Fax charges apply) If you fax in your |
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
Express Service Fee |
|
$15.00ea |
|
|
|
application please do not mail the original. WEBETEST© High |
|
|
|
|
|
||
|
|
|
|
|
|
|
|
Volume users Internet electronic application submission. |
|
|
No Show |
|
No |
|
|
Call |
|
|
|
|
Refund |
|
|
|
|
Reschedule |
|
$35.00 |
|
|
|
CHECKS. Candidates may ONLY send cashiers check, money |
|
|
|
|
|
||
|
|
|
|
|
|
|
|
order, or use Visa/MC. Mail to PO Box 6609 Helena, MT 59604. |
|
|
Cancellation |
|
$25.00 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Grand Total Enclosed $_________ |
|||
|
|
|
|
|
|
|
|
If Facility paid then Facility name and address_____________________________________________________________________
Credit Card # (Visa, MC)___________________________________________________Expiration Date ___________/___________
Name as it appears on credit card ________________________________ Authorized Signature __________________________
Candidates CURRENTLY EMPLOYED, AS NURSE AIDES IN SKILLED MEDICARE/MEDICAID FACILITIES THAT ARE PARTIALLY REIMBURSED BY OKDH DO NOT INCLUDE FULL PAYMENT. Please call OKDH for questions about reimbursement status. Must list the Name and Location of the reimbursed Facility
Facility name and address_____________________________________________________________________________________________________
Phone (______)
The submission of this application certifies that Testing Services are requested for the candidates included. D&SDT is hereby authorized to proceed with testing and the applicant(s) understand(s) and agree(s) to abide by D&SDT testing, retesting, scheduling, rescheduling, cancellation, and No show policies.
Authorization Signature________________________________ Print Name_________________________________Phone (_____)
FORM 1402 OK |
Updated: 11/16/2005 |