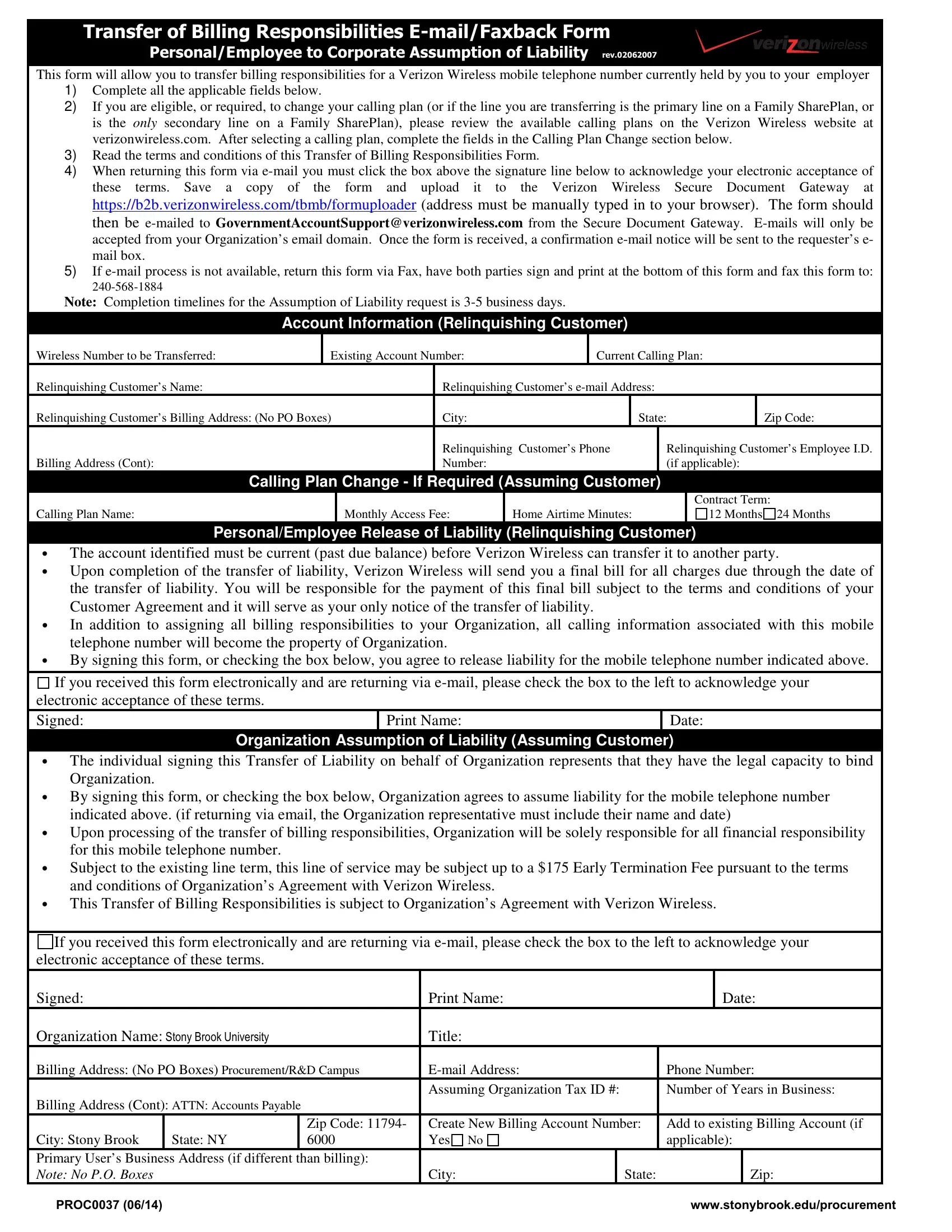
Understanding the complexities of changing billing responsibilities for a Verizon Wireless mobile telephone number is crucial for both individuals and organizations involved in this process. The Proc0037 form serves as a vital tool, designed to facilitate the transfer of billing responsibilities from an individual currently holding a Verizon account to their employer. This procedure requires careful completion of all relevant sections within the form, including personal account information, decision-making regarding potential calling plan changes, and acknowledgment of terms and conditions associated with the transfer. Notably, the process involves detailed steps for returning the form, either electronically through a secured pathway or via fax, along with the stipulation that all communication must originate from the organization's official email domain to ensure security and authenticity. The form also outlines the conditions under which the transfer can occur, such as the necessity for the account to be current without any past due balance, and the implications for both parties post-transfer, including the assumption of financial responsibility by the organization and the final bill settlement by the individual. Additionally, consideration must be given to early termination fees and adherence to Verizon's contractual terms. This overview not only highlights the procedural aspects but also underscores the mutual consent required by both parties to successfully navigate the transition, ensuring a smooth and clear transfer of liabilities and responsibilities.
| Question | Answer |
|---|---|
| Form Name | Form Proc0037 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | PROC0037 verizon transfer of billing responsibilities e mail form |
