
In case you want to fill out pamf online, you won't have to download and install any kind of applications - simply make use of our online PDF editor. To make our editor better and simpler to utilize, we consistently design new features, taking into account feedback from our users. Starting is effortless! All you need to do is take the next basic steps directly below:
Step 1: Access the PDF inside our editor by clicking the "Get Form Button" above on this webpage.
Step 2: Using this state-of-the-art PDF editor, it's possible to do more than simply fill out blanks. Express yourself and make your forms seem high-quality with custom textual content incorporated, or tweak the original input to excellence - all comes with an ability to incorporate any images and sign the file off.
This form will require some specific details; in order to ensure accuracy and reliability, don't hesitate to consider the following recommendations:
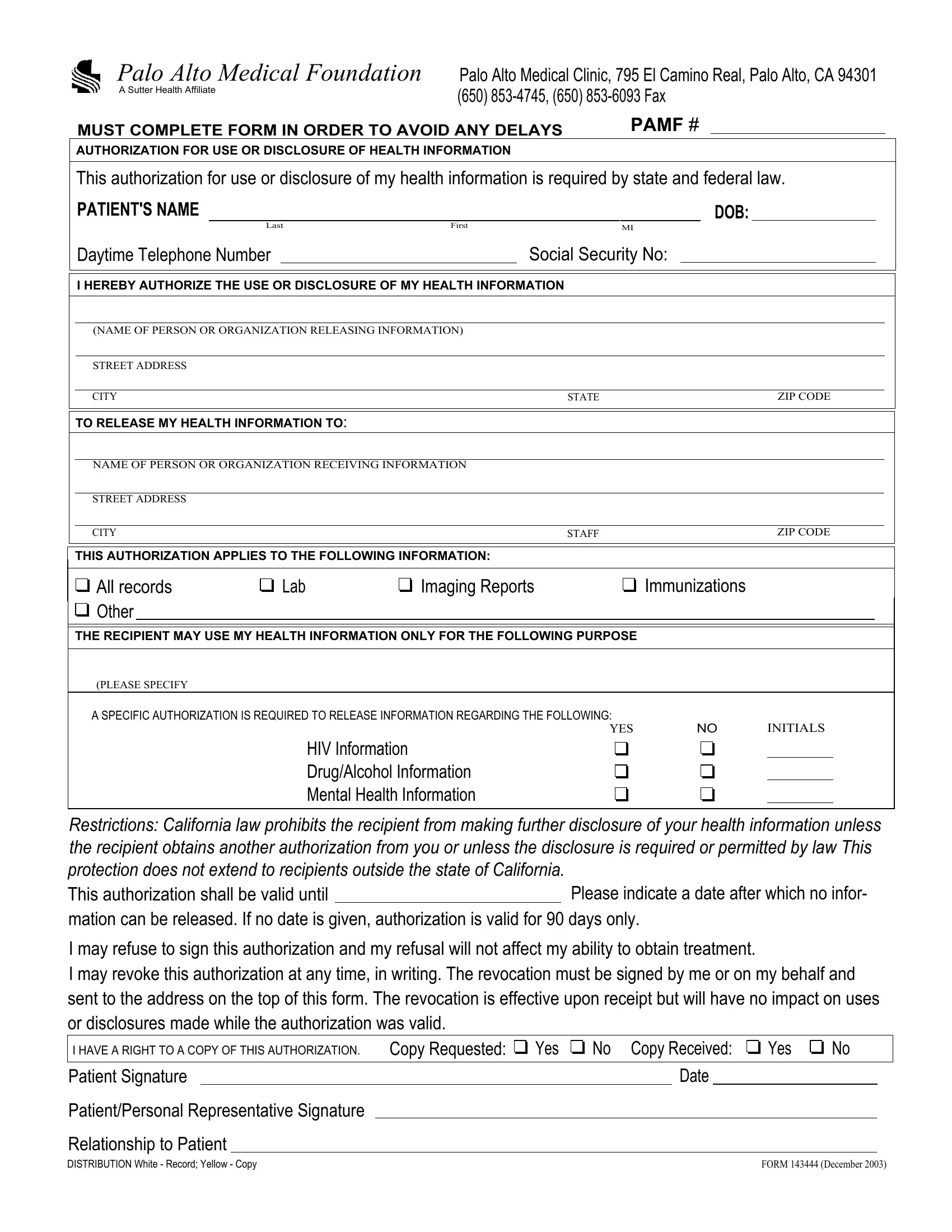
1. First, once completing the pamf online, begin with the page with the following fields:

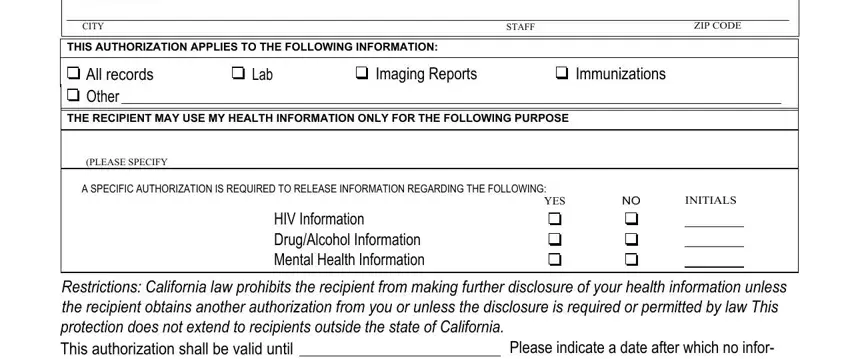
2. The third part is to submit these fields: STREET ADDRESS, CITY, STAFF, ZIP CODE, THIS AUTHORIZATION APPLIES TO THE, All records Other, Lab, Imaging Reports, Immunizations, THE RECIPIENT MAY USE MY HEALTH, PLEASE SPECIFY, A SPECIFIC AUTHORIZATION IS, YES, INITIALS, and HIV Information DrugAlcohol.
3. In this particular part, look at I may refuse to sign this, I HAVE A RIGHT TO A COPY OF THIS, Copy Requested, Yes, No Copy Received, Yes, Patient Signature, PatientPersonal Representative, Relationship to Patient, Date, and FORM December. Each of these must be taken care of with highest precision.
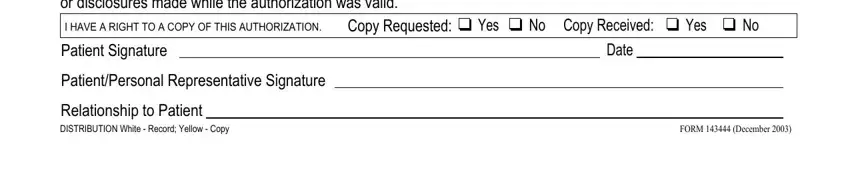
In terms of FORM December and Date, be sure that you do everything right in this section. The two of these are the key fields in this form.
Step 3: Check that your details are right and then just click "Done" to continue further. Join FormsPal right now and immediately get access to pamf online, available for download. All changes made by you are saved , so that you can modify the pdf further as needed. We don't sell or share any information you type in when filling out documents at our website.