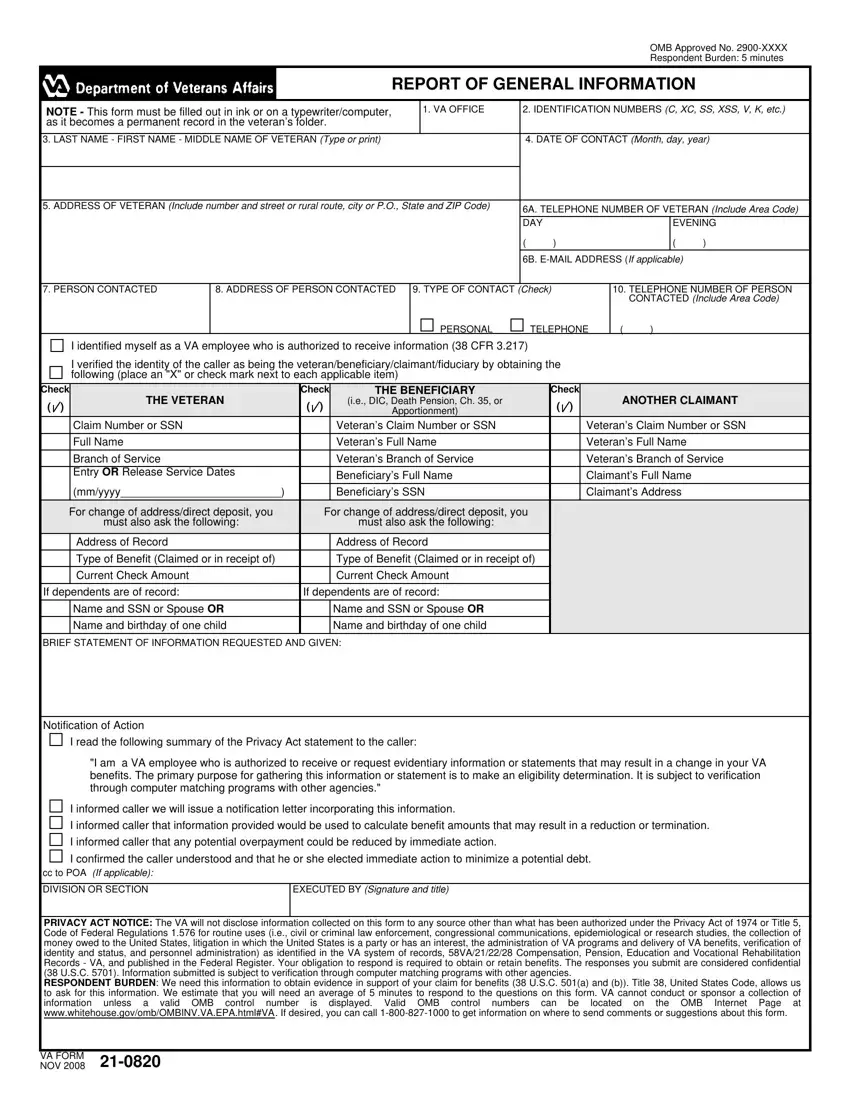
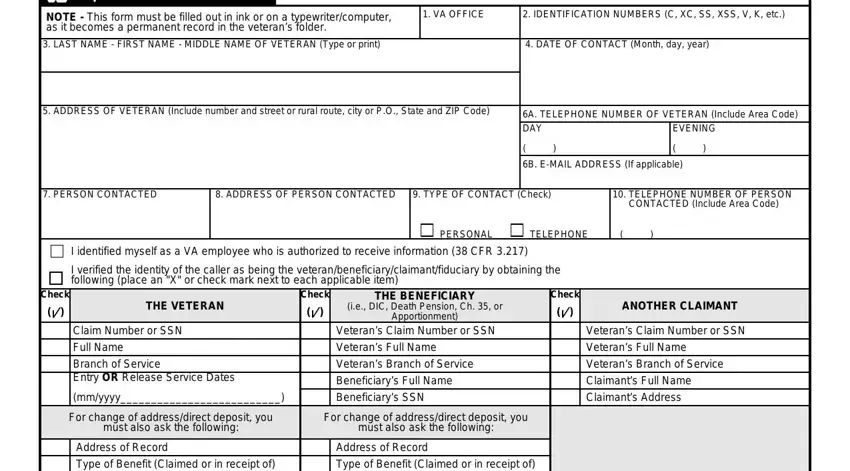
I identified myself as a VA employee who is authorized to receive information (38 CFR 3.217)
I verified the identity of the caller as being the veteran/beneficiary/claimant/fiduciary by obtaining the following (place an "X" or check mark next to each applicable item)
Check |
THE VETERAN |
Check |
THE BENEFICIARY |
Check |
ANOTHER CLAIMANT |
( |
|
) |
|
( |
|
) |
(i.e., DIC, Death Pension, Ch. 35, or |
( |
|
) |
|
|
|
|
Apportionment) |
|
|
|
|
|
|
Claim Number or SSN |
|
|
|
Veteran's Claim Number or SSN |
|
|
|
Veteran's Claim Number or SSN |
|
|
|
|
Full Name |
|
|
|
Veteran's Full Name |
|
|
|
Veteran's Full Name |
|
|
|
|
Branch of Service |
|
|
|
Veteran's Branch of Service |
|
|
|
Veteran's Branch of Service |
|
|
|
|
Entry OR Release Service Dates |
|
|
|
Beneficiary's Full Name |
|
|
|
Claimant's Full Name |
|
|
|
|
(mm/yyyy__________________________) |
|
|
|
Beneficiary's SSN |
|
|
|
Claimant's Address |
|
|
|
For change of address/direct deposit, you |
|
|
For change of address/direct deposit, you |
|
|
|
|
|
|
|
|
must also ask the following: |
|
|
|
must also ask the following: |
|
|
|
|
|
|
|
|
Address of Record |
|
|
|
Address of Record |
|
|
|
|
|
|
|
|
Type of Benefit (Claimed or in receipt of) |
|
|
|
Type of Benefit (Claimed or in receipt of) |
|
|
|
|
|
|
|
|
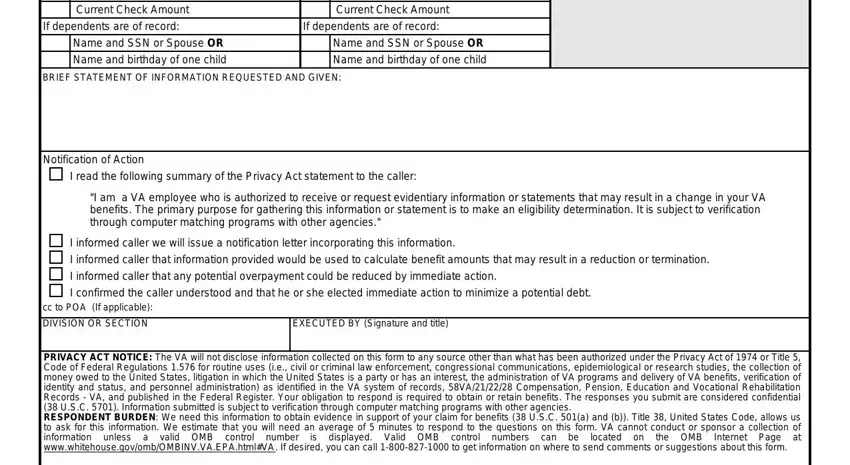
Current Check Amount |
|
|
|
Current Check Amount |
|
|
|
|
If dependents are of record: |
If dependents are of record: |
|
|
|
|
|
|
|
|
Name and SSN or Spouse OR |
|
|
|
Name and SSN or Spouse OR |
|
|
|
|
|
|
|
|
Name and birthday of one child |
|
|
|
Name and birthday of one child |
|
|
|
|
BRIEF STATEMENT OF INFORMATION REQUESTED AND GIVEN:
Notification of Action
I read the following summary of the Privacy Act statement to the caller:
"I am a VA employee who is authorized to receive or request evidentiary information or statements that may result in a change in your VA benefits. The primary purpose for gathering this information or statement is to make an eligibility determination. It is subject to verification through computer matching programs with other agencies."
I informed caller we will issue a notification letter incorporating this information.
I informed caller that information provided would be used to calculate benefit amounts that may result in a reduction or termination.
I informed caller that any potential overpayment could be reduced by immediate action.
I confirmed the caller understood and that he or she elected immediate action to minimize a potential debt.
ccto POA (If applicable):
DIVISION OR SECTION |
EXECUTED BY (Signature and title) |
|
|
PRIVACY ACT NOTICE: The VA will not disclose information collected on this form to any source other than what has been authorized under the Privacy Act of 1974 or Title 5, Code of Federal Regulations 1.576 for routine uses (i.e., civil or criminal law enforcement, congressional communications, epidemiological or research studies, the collection of money owed to the United States, litigation in which the United States is a party or has an interest, the administration of VA programs and delivery of VA benefits, verification of identity and status, and personnel administration) as identified in the VA system of records, 58VA/21/22/28 Compensation, Pension, Education and Vocational Rehabilitation Records - VA, and published in the Federal Register. Your obligation to respond is required to obtain or retain benefits. The responses you submit are considered confidential (38 U.S.C. 5701). Information submitted is subject to verification through computer matching programs with other agencies.
RESPONDENT BURDEN: We need this information to obtain evidence in support of your claim for benefits (38 U.S.C. 501(a) and (b)). Title 38, United States Code, allows us to ask for this information. We estimate that you will need an average of 5 minutes to respond to the questions on this form. VA cannot conduct or sponsor a collection of information unless a valid OMB control number is displayed. Valid OMB control numbers can be located on the OMB Internet Page at www.whitehouse.gov/omb/OMBINV.VA.EPA.html#VA. If desired, you can call 1-800-827-1000 to get information on where to send comments or suggestions about this form.