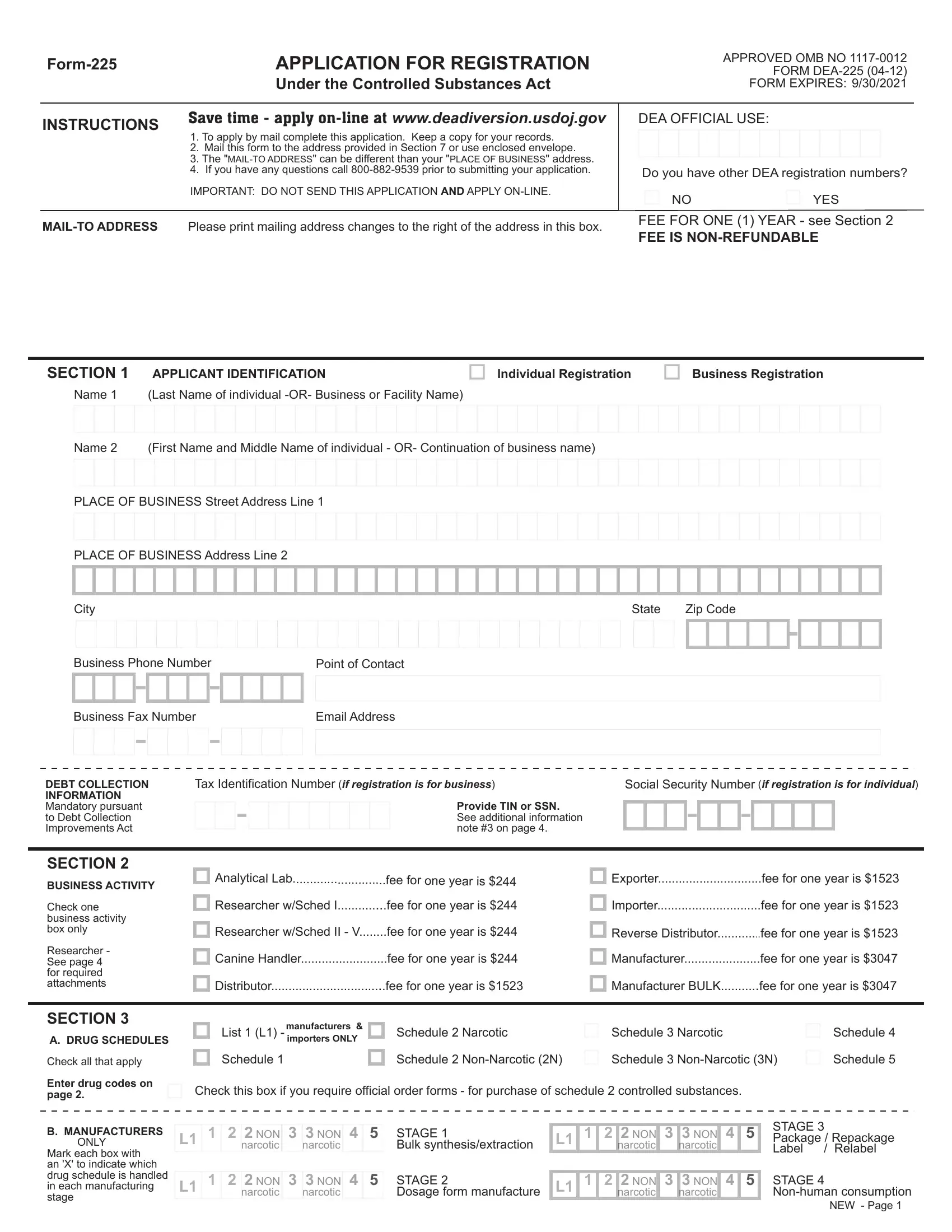
Navigating the complexities of the Controlled Substances Act (CSA) often culminates in the encounter with Form DEA-225, an essential vehicle for entities aiming to lawfully engage with controlled substances. This form serves as a beacon for researchers, manufacturers, distributors, and others by delineating the procedural roadmap for registration under the CSA. The detailed sections of the form intricately lay out the necessities — from applicant identification to business activities, schedules, and drug codes. It mandates specific attention to liability questions, a consequential area given the legal and ethical ramifications tied to controlled substance management. Moreover, the division regarding state licenses underscores the dual necessity of adhering to both federal and state regulatory frameworks — a symbiotic legal relationship often navigated with caution. The financial aspect, as indicated by the non-refundable fees, the option for exemption, and the explicit instruction for selecting a payment method, alongside the solemn declaration required in the applicant’s signature, concretizes the formal engagement with the DEA. The form not only facilitates compliance with regulatory mandates but also embodies the multifaceted considerations spanning legal statutes, ethical considerations, and administrative logistics integral to controlled substance research, distribution, or manufacturing.
| Question | Answer |
|---|---|
| Form Name | Form 225 |
| Form Length | 4 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min |
| Other names | dea, dea 225 form 225 substance, form 225 application, form 225 application control substance |