NICS (National Instant Criminal Background Check System) is a system that is used to determine whether or not a gun buyer is eligible to purchase a firearm. Form 24 NCIC is the form that must be completed by the gun buyer and submitted to the FBI in order to initiate the NICS background check. Completing this form accurately and submitting it on time is essential for ensuring a smooth and timely purchase process. Our blog post today will provide all of the details you need to know about Form 24 NCIC, including who needs to fill it out and when it should be submitted. Stay tuned for more helpful tips on purchasing firearms!
| Question | Answer |
|---|---|
| Form Name | Form 24 Ncic |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | HTTP, WWW, RALEIGH, indemnity |
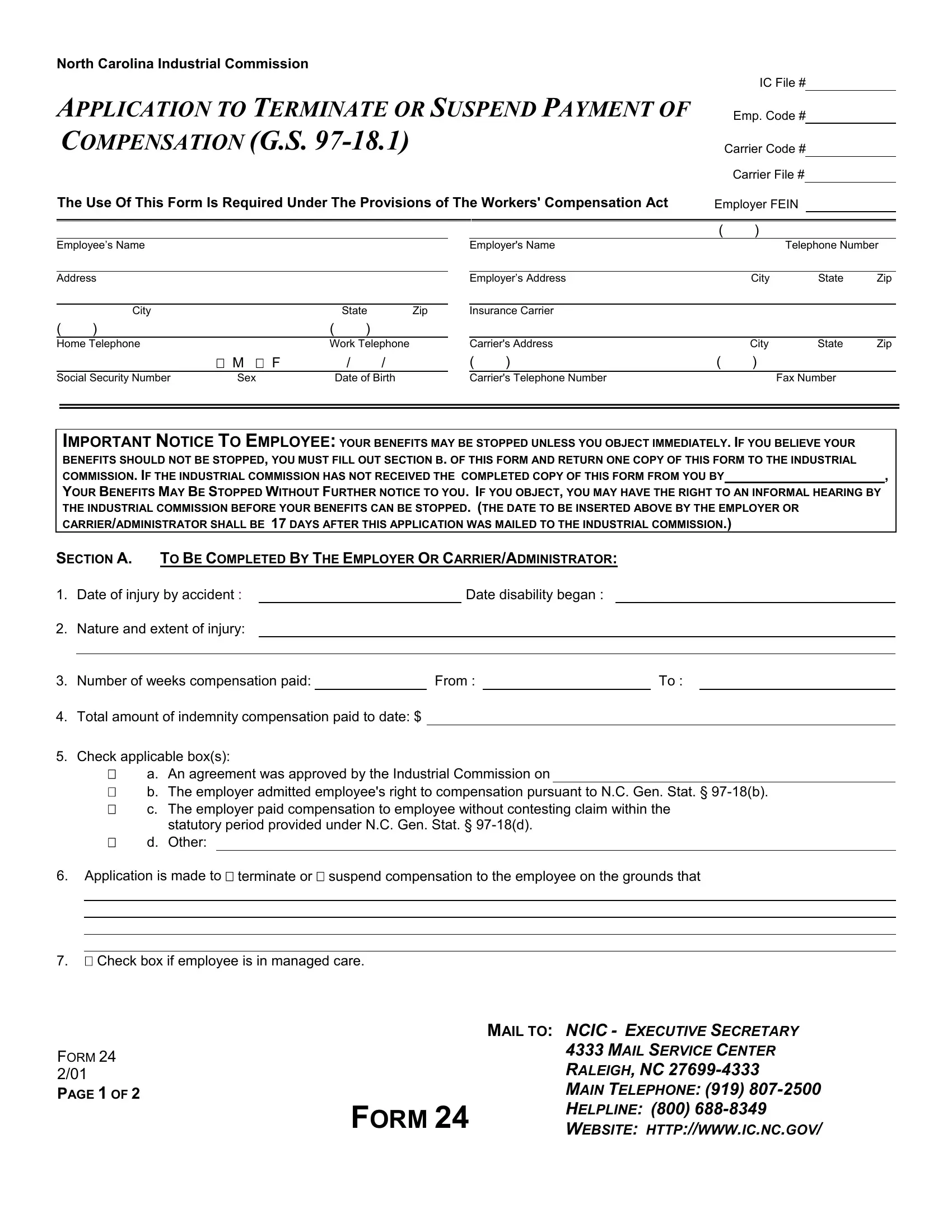
North Carolina Industrial Commission
IC File #
APPLICATION TO TERMINATE OR SUSPEND PAYMENT OF
COMPENSATION (G.S.
Emp. Code #
Carrier Code # Carrier File #
The Use Of This Form Is Required Under The Provisions of The Workers' Compensation Act |
Employer FEIN |
Employee’s Name
Address
|
City |
|
|
State |
Zip |
( |
) |
|
( |
) |
|
Home Telephone |
|
Work Telephone |
|||
|
|
M F |
|
/ |
/ |
Social Security Number |
Sex |
|
Date of Birth |
||
|
|
( |
) |
|
|
Employer's Name |
|
|
Telephone Number |
||
|
|
|
|
|
|
Employer’s Address |
|
City |
State |
Zip |
|
|
|
|
|
|
|
Insurance Carrier |
|
|
|
|
|
|
|
|
|
|
|
Carrier's Address |
|
City |
State |
Zip |
|
( |
) |
( |
) |
|
|
Carrier's Telephone Number |
|
|
Fax Number |
|
|
IMPORTANT NOTICE TO EMPLOYEE: YOUR BENEFITS MAY BE STOPPED UNLESS YOU OBJECT IMMEDIATELY. IF YOU BELIEVE YOUR |
|
BENEFITS SHOULD NOT BE STOPPED, YOU MUST FILL OUT SECTION B. OF THIS FORM AND RETURN ONE COPY OF THIS FORM TO THE INDUSTRIAL |
|
COMMISSION. IF THE INDUSTRIAL COMMISSION HAS NOT RECEIVED THE COMPLETED COPY OF THIS FORM FROM YOU BY |
, |
YOUR BENEFITS MAY BE STOPPED WITHOUT FURTHER NOTICE TO YOU. IF YOU OBJECT, YOU MAY HAVE THE RIGHT TO AN INFORMAL HEARING BY THE INDUSTRIAL COMMISSION BEFORE YOUR BENEFITS CAN BE STOPPED. (THE DATE TO BE INSERTED ABOVE BY THE EMPLOYER OR CARRIER/ADMINISTRATOR SHALL BE 17 DAYS AFTER THIS APPLICATION WAS MAILED TO THE INDUSTRIAL COMMISSION.)
SECTION A. TO BE COMPLETED BY THE EMPLOYER OR CARRIER/ADMINISTRATOR:
1. |
Date of injury by accident : |
|
|
|
Date disability began : |
|
|
|
|
2. |
Nature and extent of injury: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
3. |
Number of weeks compensation paid: |
|
From : |
|
|
To : |
|
||
4.Total amount of indemnity compensation paid to date: $
5.Check applicable box(s):
a. An agreement was approved by the Industrial Commission on
b. The employer admitted employee's right to compensation pursuant to N.C. Gen. Stat. §
c. The employer paid compensation to employee without contesting claim within the
statutory period provided under N.C. Gen. Stat. §
d. Other:
6.Application is made to terminate or suspend compensation to the employee on the grounds that
7. Check box if employee is in managed care.
|
MAIL TO: NCIC - EXECUTIVE SECRETARY |
|
FORM 24 |
4333 MAIL SERVICE CENTER |
|
RALEIGH, NC |
||
2/01 |
||
PAGE 1 OF 2 |
MAIN TELEPHONE: (919) |
|
FORM 24 |
HELPLINE: (800) |
|
WEBSITE: HTTP://WWW.IC.NC.GOV/ |
In addition to filing the original of this application and supporting documents with the Industrial Commission, I hereby certify that a copy of this application, together with all supporting documents, was mailed to the employee at
(address) |
|
|
|
|
|||
|
|
|
|
|
|
|
|
and employee's attorney of record, if any, on |
|
|
. |
|
|
||
The attached documents consist of |
|
(number) pages. |
|
|
|||
|
|
|
|
||||
SIGNATURE OF EMPLOYER OR CARRIER/ADMINISTRATOR |
PRINTED NAME |
TELEPHONE NUMBER |
DATE |
||||
TO BE COMPLETED BY THE EMPLOYEE
SECTION B. IF YOU THINK YOUR COMPENSATION SHOULD NOT BE STOPPED, YOU SHOULD COMPLETE THIS SECTION.
1.I do not think my compensation should be stopped because:
2.Enclose and specify the number of pages of documents the Industrial Commission should consider: (number).
3.Give a telephone number at which you can be reached when the informal hearing is scheduled, from Monday through Friday
between 8:00 a.m. and 5:00 p.m.: |
|
. The Industrial Commission will notify you of the date and time of the hearing. |
SIGNATURE OF EMPLOYEE |
WITNESS |
DATE |
If you need assistance in completing this form, you may contact the Industrial Commission at (800)
Office of the Executive Secretary at (919)
documents you have not been able to obtain.
EMPLOYEE: SEND A COPY OF THIS FORM AND SUPPORTING DOCUMENTS TO THE EMPLOYER AND
CARRIER/ADMINISTRATOR FROM WHOM YOU ARE RECEIVING COMPENSATION. SEND THE ORIGINAL TO:
INDUSTRIAL COMMISSION, OFFICE OF THE EXECUTIVE SECRETARY, 4333 MAIL SERVICE CENTER, RALEIGH NC
|
MAIL TO: NCIC - EXECUTIVE SECRETARY |
|
FORM 24 |
4333 MAIL SERVICE CENTER |
|
RALEIGH, NC |
||
2/01 |
||
PAGE 2 OF 2 |
MAIN TELEPHONE: (919) |
|
FORM 24 |
HELPLINE: (800) |
|
WEBSITE: HTTP://WWW.IC.NC.GOV/ |