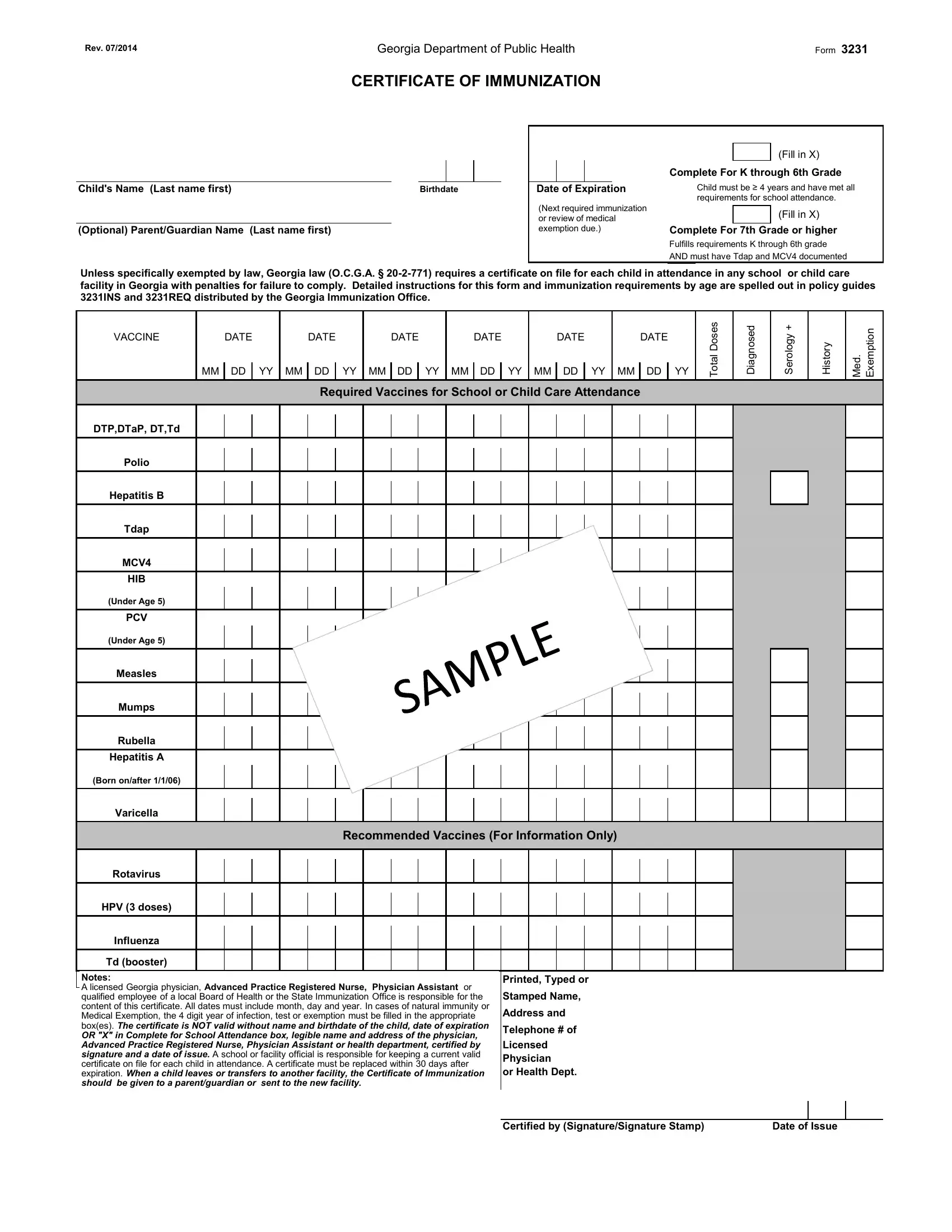
Ensuring that children are vaccinated according to state laws is a paramount responsibility for parents and guardians, a task where the Georgia Department of Public Health Form 3231 plays a crucial role. This Certificate of Immunization is a comprehensive document that records a child's vaccination history, a requirement for enrollment in any school or childcare facility across Georgia. Not only does it list mandatory vaccines such as DTP, DTaP, DT, Td Polio, Hepatitis B, Tdap, MCV4, among others for school or childcare attendance, but it also mentions vaccines recommended for optimal health. Form 3231, last revised in July 2014, mandates inclusion of the child's name, birthdate, and the parent or guardian's name, alongside the vaccination dates, making it a personalized immunization record. It stipulates requirements for children entering K through 6th grade and those in 7th grade or higher, reflecting the state's commitment to public health through vaccination. The form also accommodates medical exemptions, should they exist, with specific sections for diagnosed serology plus history, and details any medical exemptions, thereby enshrining in policy understanding and flexibility for individual health needs and considerations. Compliance is not merely encouraged but required under Georgia law (O.C.G.A. § 20-2-771), with penalties for failure to comply, emphasizing the seriousness with which the state regards this aspect of public health. The logistical aspects of maintaining, updating, and transferring these records are also outlined, ensuring that each child's vaccination record is current, accessible, and within legal compliance at all times. Thus, Form 3231 serves not only as a record but also as a critical checkpoint in the safeguarding of public health in educational and childcare settings across Georgia.
| Question | Answer |
|---|---|
| Form Name | Form 3231 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | ga form 3231 printable, ga form 3231, form 3231 pdf, form 3231 georgia |
