
 N
N
Our top rated programmers worked hard to design the PDF editor we are now pleased to present to you. Our software permits you to easily prepare 3613a and will save you valuable time. You need to simply comply with this particular guide.
Step 1: Click the "Get Form Here" button.
Step 2: You are now on the form editing page. You can edit, add information, highlight certain words or phrases, insert crosses or checks, and add images.
Type in the essential material in every segment to create the PDF 3613a
Indicate the information in Street Address, City State ZIP Code, County, Area Code and Telephone No, Fax Area Code and Telephone No, Parent, BranchAlternate Delivery Site, Confidential Document, This communication including any, Use only for Skilled Nursing, and Form A.
Note the necessary data in DADS Intake ID No, Date Reported to DADS, Vendor ID No, Time Reported, Telephone No Fax, City, ZIP Code, Drug Diversion Fire Alarm Failure, Fire, Bomb Threat Firearms in the, Provider Type, Name, Street Address, Incident Category, and Abuse field.
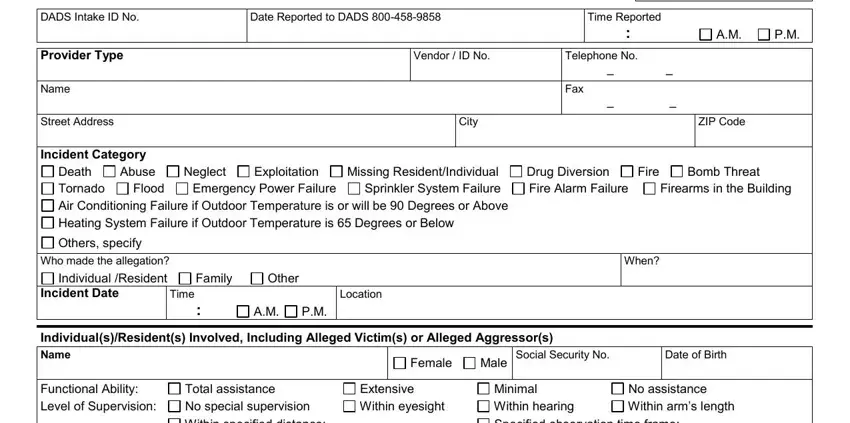
The Total assistance No special, Minimal Within hearing Specified, Other, Independently ambulatory History of, Interviewable Verbal aggression, N Capacity to make informed, Physical aggression, Sexual misconduct, Wearing wander guard at time of, Similar allegations, Combativeness Wandering, Other pertinent history, Name, Female, and Male field will be the place to put the rights and obligations of both parties.
Look at the fields Combativeness Wandering, Other pertinent history, Wearing wander guard at time of, and Similar allegations and then complete them.

Step 3: After you select the Done button, your finished document can be easily transferred to all of your devices or to electronic mail provided by you.
Step 4: To prevent different problems in the long run, be sure to prepare at least several duplicates of the file.
