Managing the Providers document is not hard with our PDF editor. Stick to these actions to prepare the document straight away.
Step 1: Choose the "Get Form Here" button.
Step 2: So you are on the file editing page. You may edit and add text to the document, highlight specified content, cross or check selected words, include images, insert a signature on it, erase unwanted areas, or eliminate them entirely.
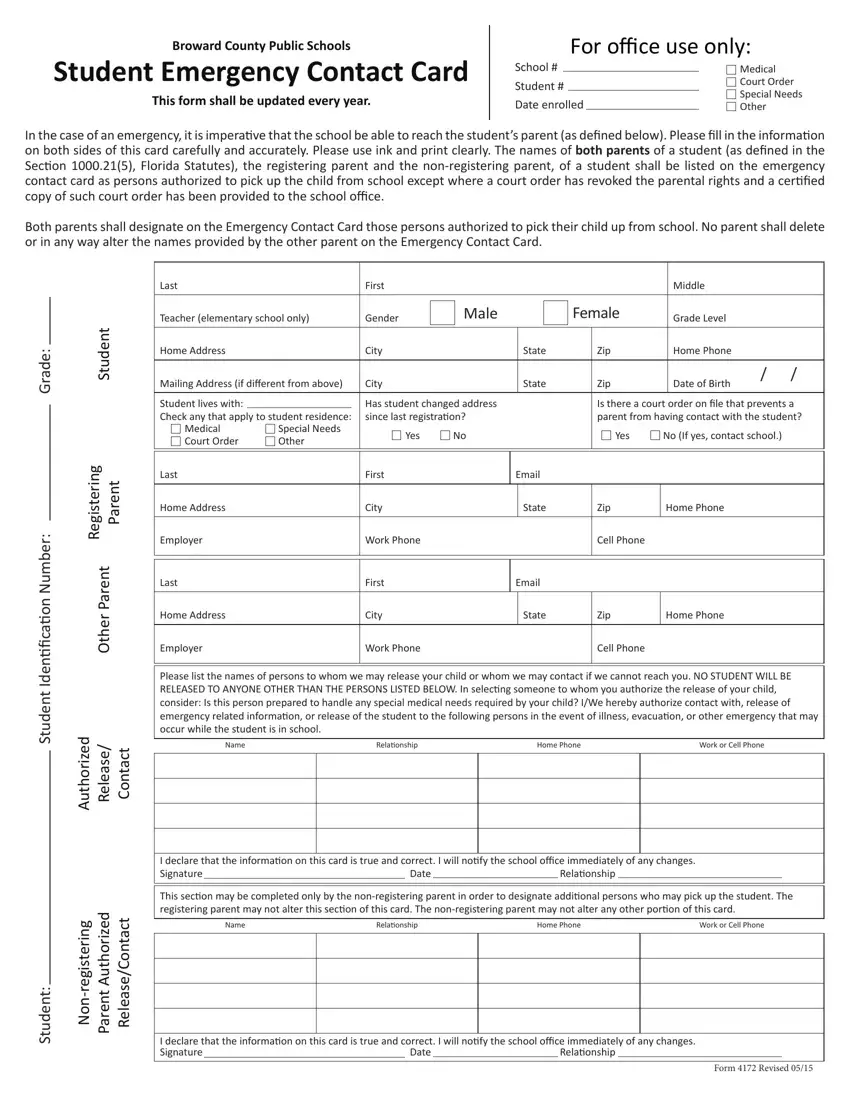
Fill out the Providers PDF and provide the details for every single part:
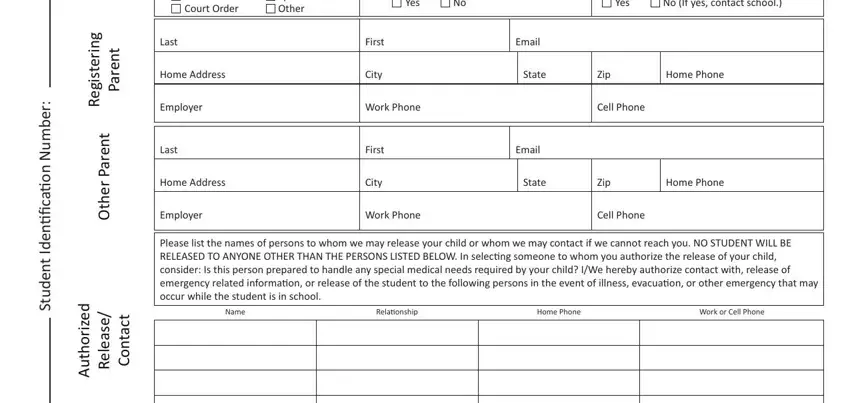
Complete the g n i r e t s i g e R, t n e r a P, t n e r a P r e h t O, d e z i r o h t u A, e s a e e R, t c a t n o C, r e b m u N n o i a c i i n e d, t n e d u t S, Medical Court Order, Special Needs Other, Yes, Yes, No If yes contact school, Last, and Home Address fields with any data that can be demanded by the system.
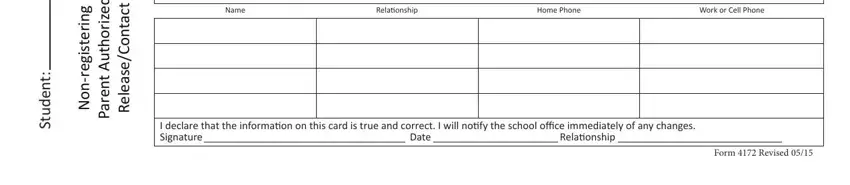
Outline the relevant data in the g n i r e t s i g e r n o N, d e z i r o h t u A t n e r a P, t c a t n o C e s a e e R, t n e d u t S, This secion may be completed only, Name, Relaionship, Home Phone, Work or Cell Phone, I declare that the informaion on, Date, Relaionship, and Form Revised section.
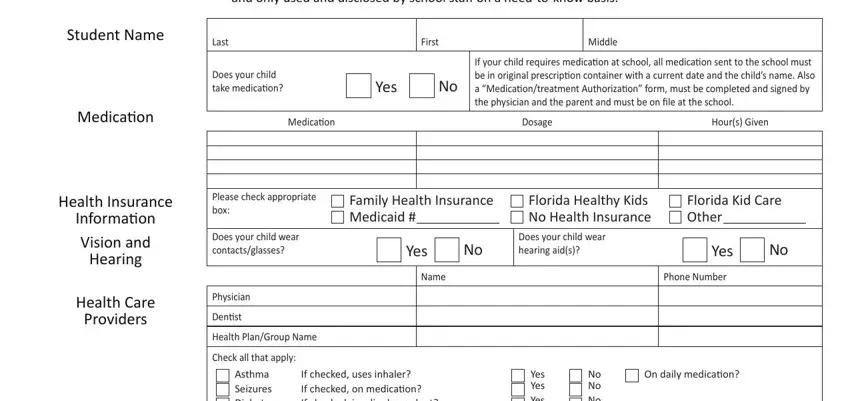
The The personal informaion you, Student Name, Last, First, Middle, Does your child take medicaion, Yes, If your child requires medicaion, Medicaion, Medicaion, Dosage, Hours Given, Health Insurance Informaion Vision, Please check appropriate box, and Does your child wear section is where all parties can describe their rights and responsibilities.
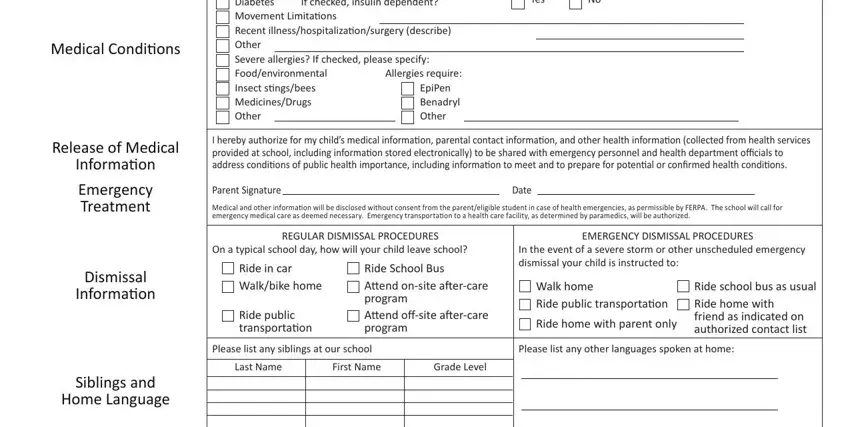
End by analyzing all of these sections and typing in the required data: If checked uses inhaler If checked, Check all that apply Asthma, EpiPen Benadryl Other, Allergies require, Yes Yes Yes, No No No, I hereby authorize for my childs, Parent Signature, Date, Medical and other informaion will, REGULAR DISMISSAL PROCEDURES, EMERGENCY DISMISSAL PROCEDURES, On a typical school day how will, Ride in car Walkbike home, and Ride public transportaion.
Step 3: Hit the "Done" button. So now, you can transfer the PDF document - download it to your electronic device or deliver it by means of email.
Step 4: Come up with no less than a couple of copies of the form to keep clear of any kind of potential future issues.
