The form known as "45" plays a pivotal role in the support system for relative care arrangements, embodying an application and agreement process for accessing Relative Care Subsidy (RCS) and its enhanced variant. This document sets the stage for a vital financial aid designed to support relatives who have taken on the commendable responsibility of caring for a family member's child, ensuring the child's welfare following a court's decision to assign legal custody. The form meticulously outlines the prerequisites for income verification, the agreement's effective period, renewal stipulations, and the comprehensive terms and conditions tied to the subsidy. By signing, caregivers pledge to provide a secure, stable, and nurturing environment that caters to the child's diverse needs — from health and emotional support to educational provisions. Furthermore, it mandates an open communication channel with the relevant Department of Human Resource and compliance with periodical reports, aiming to facilitate the child's overall well-being. The agreement delves into expectations regarding household changes, the provision of mental health services, and adhering to DFCS and court requirements, solidifying a framework for care that emphasizes the child's best interests at its core.
| Question | Answer |
|---|---|
| Form Name | Form 45 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | 18th, relative care subsidy, enhanced relative rate agreement, specifying |
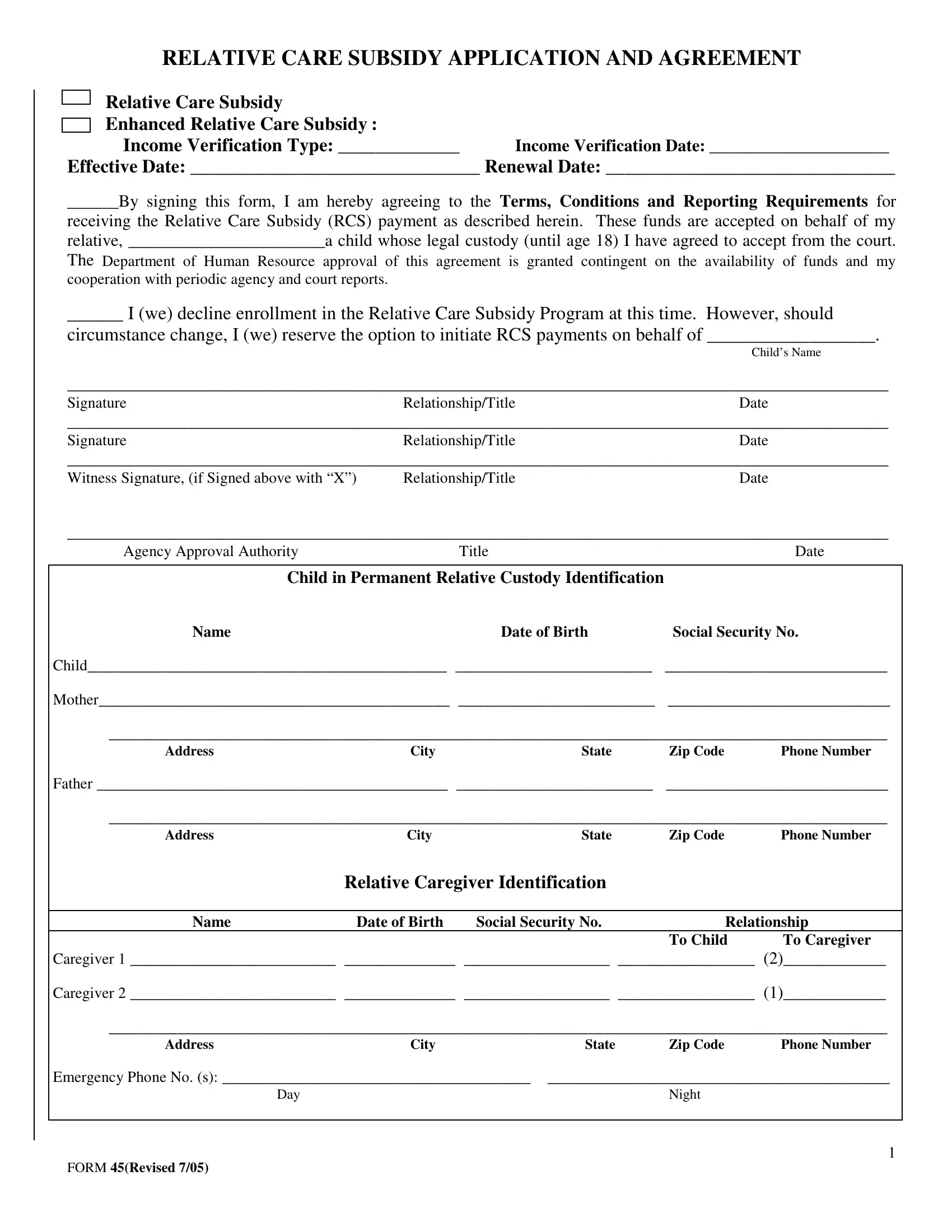
RELATIVE CARE SUBSIDY APPLICATION AND AGREEMENT
Relative Care Subsidy
Enhanced Relative Care Subsidy :
Income Verification Type: _____________ Income Verification Date: _____________________
Effective Date: _______________________________ Renewal Date: _______________________________
______By signing this form, I am hereby agreeing to the Terms, Conditions and Reporting Requirements for
receiving the Relative Care Subsidy (RCS) payment as described herein. These funds are accepted on behalf of my relative, _______________________a child whose legal custody (until age 18) I have agreed to accept from the court.
The Department of Human Resource approval of this agreement is granted contingent on the availability of funds and my cooperation with periodic agency and court reports.
______ I (we) decline enrollment in the Relative Care Subsidy Program at this time. However, should
circumstance change, I (we) reserve the option to initiate RCS payments on behalf of __________________.
Child’s Name
________________________________________________________________________________________________
SignatureRelationship/TitleDate
________________________________________________________________________________________________
SignatureRelationship/TitleDate
________________________________________________________________________________________________
Witness Signature, (if Signed above with “X”) Relationship/TitleDate
________________________________________________________________________________________________
Agency Approval Authority |
|
Title |
|
Date |
|
|
|
||
Child in Permanent Relative Custody Identification |
|
|
||
Name |
|
Date of Birth |
Social Security No. |
|
Child__________________________________________ _______________________ |
__________________________ |
|||
Mother_________________________________________ _______________________ |
__________________________ |
|||
___________________________________________________________________________________________ |
||||
Address |
City |
State |
Zip Code |
Phone Number |
Father _________________________________________ _______________________ |
__________________________ |
|||
___________________________________________________________________________________________ |
||||
Address |
City |
State |
Zip Code |
Phone Number |
|
Relative Caregiver Identification |
|
|
|
|
|
|
|
|
Name |
Date of Birth |
Social Security No. |
Relationship |
|
|
|
|
To Child |
To Caregiver |
Caregiver 1 ________________________ _____________ _________________ ________________ (2)____________
Caregiver 2 ________________________ _____________ _________________ ________________ (1)____________
___________________________________________________________________________________________
AddressCityStateZip CodePhone Number
Emergency Phone No. (s): ____________________________________ |
________________________________________ |
Day |
Night |
|
|
|
1 |
FORM 45(Revised 7/05)
Relative Care Subsidy Terms of Agreement
I (We), _______________________________________ and ______________________________________,
am (are) committed to providing a permanent home for our relative, _________________________________,
a child in the temporary legal custody of _______________________County Department of Family and
Children Services (DFCS). In accepting this responsibility, I (we) knowingly enter into an agreement with DFCS regarding his/her overall health, care and wellbeing while in my (our) home and care. It is my (our) understanding that once the court has issued the court order awarding permanent custody to me (us), the following will apply, and we are, hereby, agreeing to these Terms and Conditions:
1.I (We) agree to provide the child with a nurturing and stable home environment.
2.I (We) agree to protect the child from harm or maltreatment.
3.I (We) agree to abide with DFCS and court requirements regarding this child’s care.
4.I (We) agree to assure that his/her health, emotional, psychosocial, educational and physical needs are met.
5.I (We) agree to provide adequate clothing, appropriate for weather conditions and child’s special needs.
6.I (We) agree to provide for child’s dietary needs and special foods or supplements required for him/her.
7.I (We) agree to seek and obtain mental health and /or counseling services recommended for the child.
8.I (We) agree to notify the agency and court of changes in the household circumstances which may affect the child, such as
a). person(s), over age 17, moving into or out of the household,
b). caregiver(s) name changes,
c). child/family moves to new address,
d). child runs away, is kidnapped or whereabouts are unknown,
e). child is seriously injured, becomes critically ill, or dies,
f). child is incarcerated and expected to be retained beyond his/her 18th birthday,
g). child marries and moves out of the home,
h). child receives personal income or benefits equivalent to or greater than the current foster care per diem rate,
i). child is removed from my home due to abuse, neglect or other maltreatment,
j). child is returned to the permanent legal custody of the birth parent(s), or
k). any circumstance causing the child to be at risk and/or no longer requiring this placement and/or this subsidy.
It is my (our) understanding that staff from ______________________________County DFCS office will do
the following (or arrange same) with the social services agency in the county where I (we) reside:
1.Send advance notification to schedule the annual review of my home.
2.Complete an annual review of my home.
3.Send me (us) written notification of the continuation (specifying the amount) or termination of the subsidy payments. The dates of the eligibility period will be included in the notification letter.
4.Provide $_______________ in monthly subsidy to help defray expenses for the child’s care.
5.Refer me (us) to service providers who are appropriate resources for addressing identified needs of the child.
I (we) understand and will abide by the court’s and agency’s expectations that I (we) will provide our young relative, __________________________________, with a safe, protective and nurturing home environment
Child’s Name
while in my(our) custody.
2
FORM 45(Revised 7/05)