
Should you intend to fill out apwu light duty request form, you don't have to download any sort of programs - simply use our online PDF editor. To make our editor better and simpler to utilize, we constantly work on new features, taking into consideration feedback from our users. To get the ball rolling, consider these easy steps:
Step 1: Just hit the "Get Form Button" at the top of this webpage to get into our pdf editor. There you will find everything that is required to fill out your document.
Step 2: The editor offers the ability to change your PDF file in a range of ways. Modify it by writing customized text, correct what's originally in the file, and put in a signature - all close at hand!
This PDF form will require specific information to be filled in, thus be certain to take your time to enter what's asked:
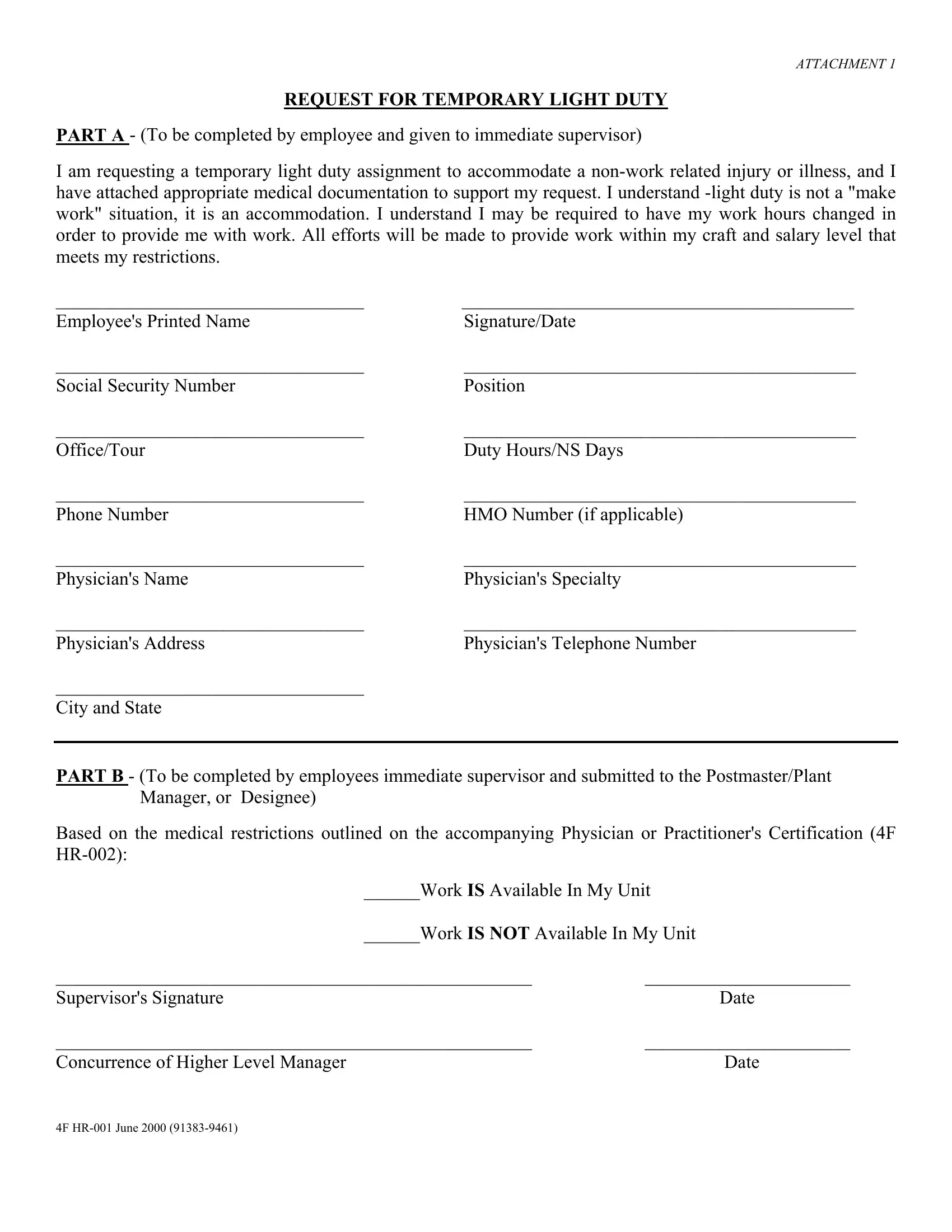
1. When completing the apwu light duty request form, make sure to complete all essential blanks within its relevant area. This will help expedite the process, which allows your details to be processed quickly and appropriately.
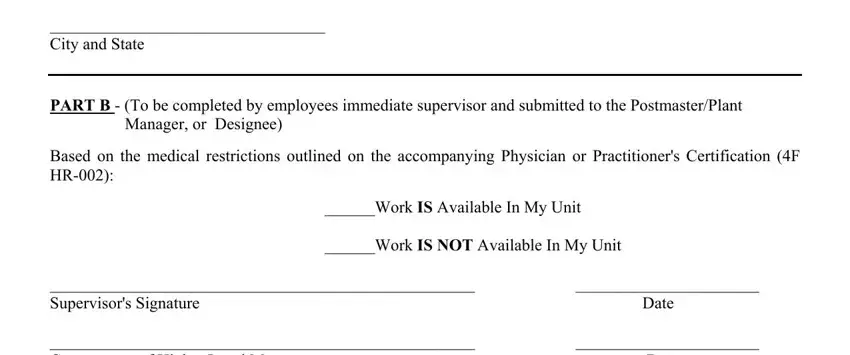
2. Soon after finishing the previous section, go on to the next step and fill out all required details in all these blank fields - PART A To be completed by, Manager or Designee, Based on the medical restrictions, Date, and Date.
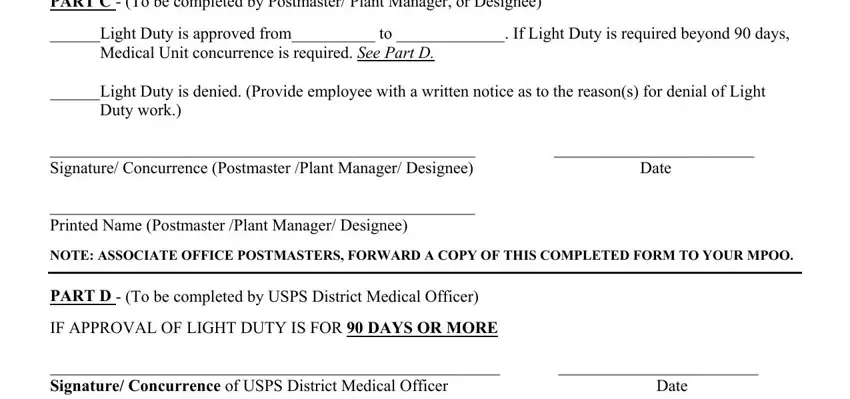
3. This next stage is generally simple - fill in every one of the blanks in REQUEST FOR TEMPORARY LIGHT DUTY, Medical Unit concurrence is, Light Duty is denied Provide, Duty work, Signature Concurrence Postmaster, and PART D To be completed by USPS in order to finish this part.
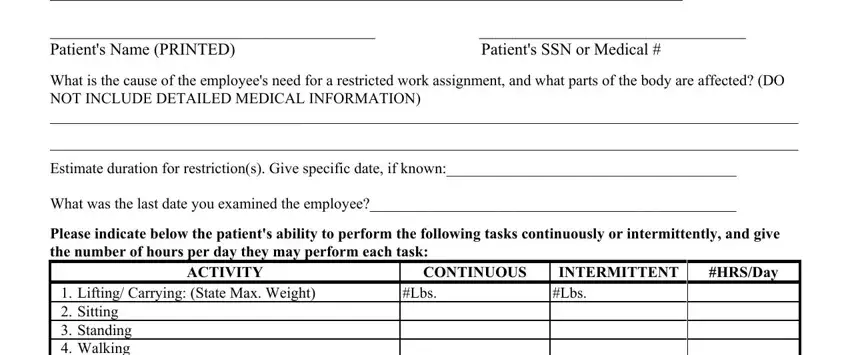
4. This next section requires some additional information. Ensure you complete all the necessary fields - PLEASE ANSWER THE FOLLOWING, Estimate duration for restrictions, HRSDay, ACTIVITY, CONTINUOUS, Lifting Carrying State Max Weight, INTERMITTENT Lbs, and Lbs - to proceed further in your process!
5. To wrap up your document, this final part has a few additional blanks. Completing Lifting Carrying State Max Weight, INTERMITTENT Lbs, Lbs, supervision meet deadlines etc Yes, and Attach any additional medical will certainly finalize everything and you'll be done in no time!
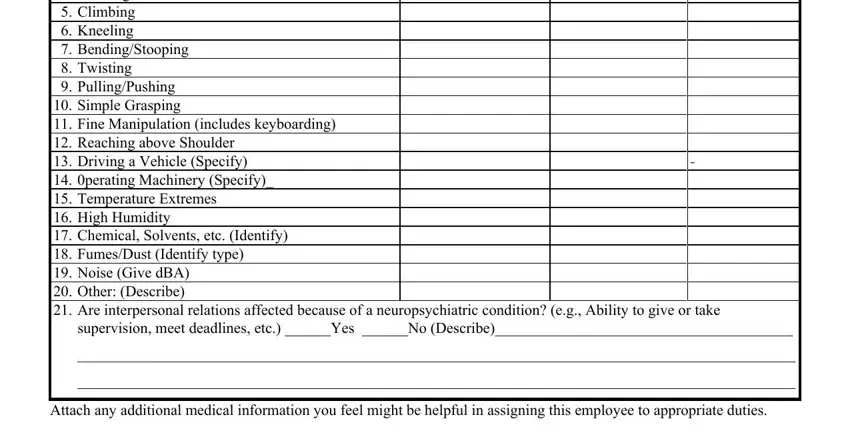
People often make errors while completing supervision meet deadlines etc Yes in this part. Be sure you go over what you enter here.
Step 3: Right after you've glanced through the details you filled in, click "Done" to finalize your document generation. Create a 7-day free trial account with us and acquire immediate access to apwu light duty request form - with all transformations saved and accessible from your FormsPal account page. FormsPal provides secure document editing devoid of data record-keeping or any sort of sharing. Feel comfortable knowing that your information is safe with us!