
You are able to prepare MTA instantly in our PDFinity® PDF editor. Our team is devoted to providing you with the absolute best experience with our tool by regularly releasing new capabilities and upgrades. With all of these updates, working with our tool gets easier than ever! All it takes is a couple of easy steps:
Step 1: Just click on the "Get Form Button" in the top section of this site to get into our pdf form editor. Here you'll find everything that is required to work with your file.
Step 2: With this handy PDF editor, it is easy to do more than merely fill out blank fields. Try each of the functions and make your documents appear professional with custom text added in, or tweak the file's original content to perfection - all backed up by the capability to incorporate any kind of graphics and sign the PDF off.
It will be an easy task to complete the document with this practical tutorial! Here's what you should do:
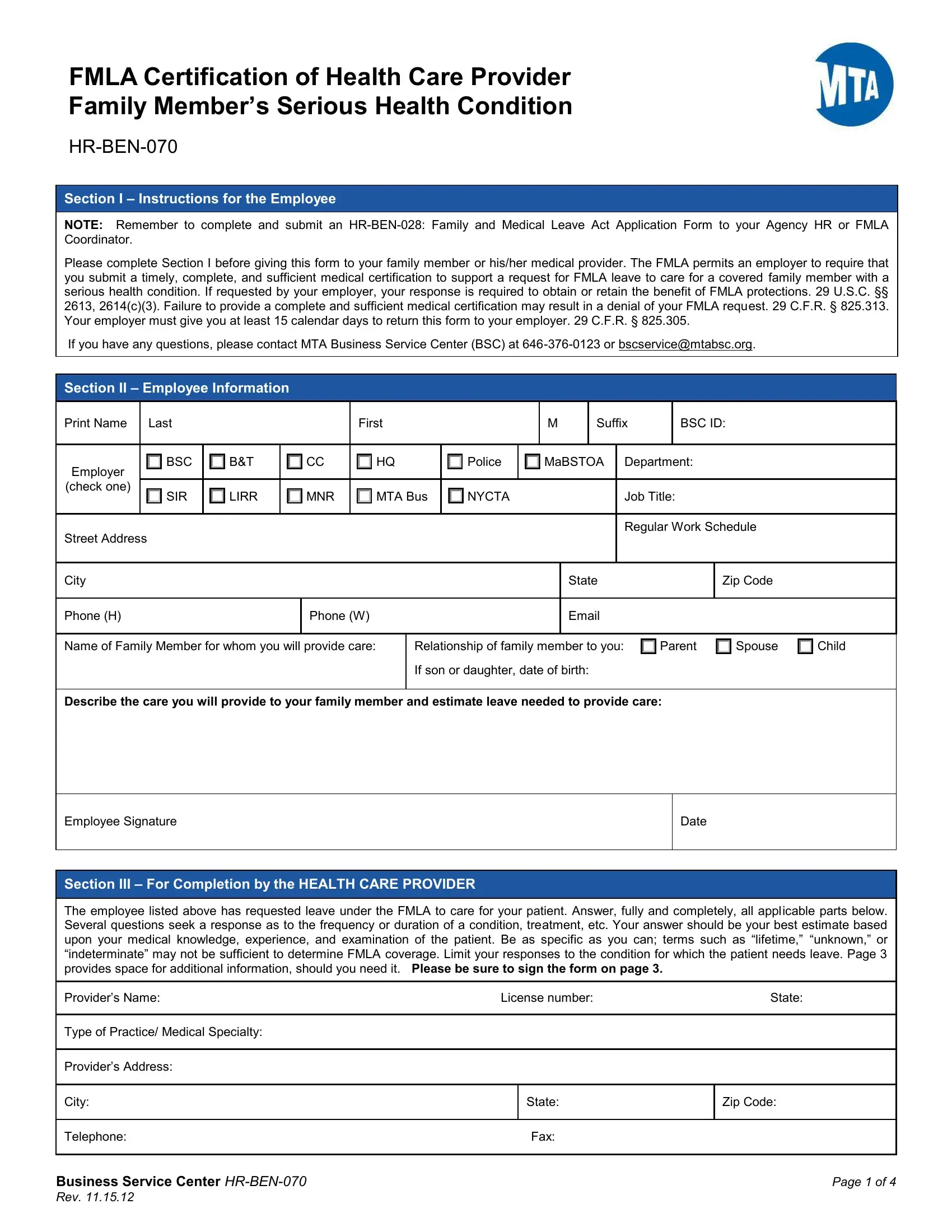
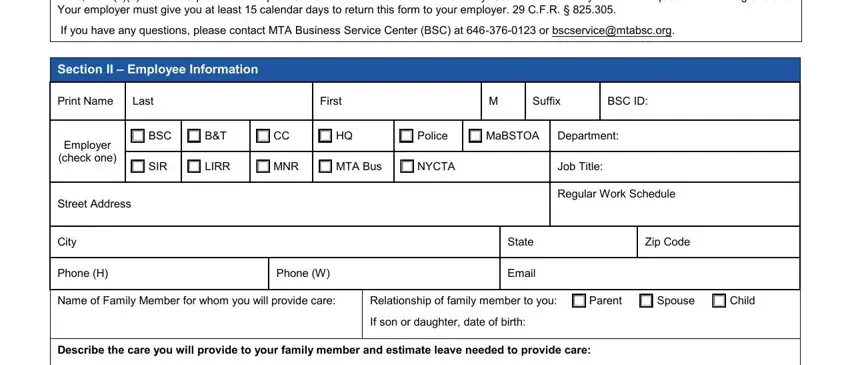
1. Begin completing the MTA with a group of necessary blank fields. Note all of the necessary information and make certain not a single thing overlooked!
2. Soon after the previous part is filled out, go on to enter the relevant information in all these - Employee Signature, Date, Section III For Completion by the, The employee listed above has, Providers Name License number State, Type of Practice Medical Specialty, Providers Address, City, State, Zip Code, Telephone Fax, Business Service Center HRBEN Rev, and Page of.
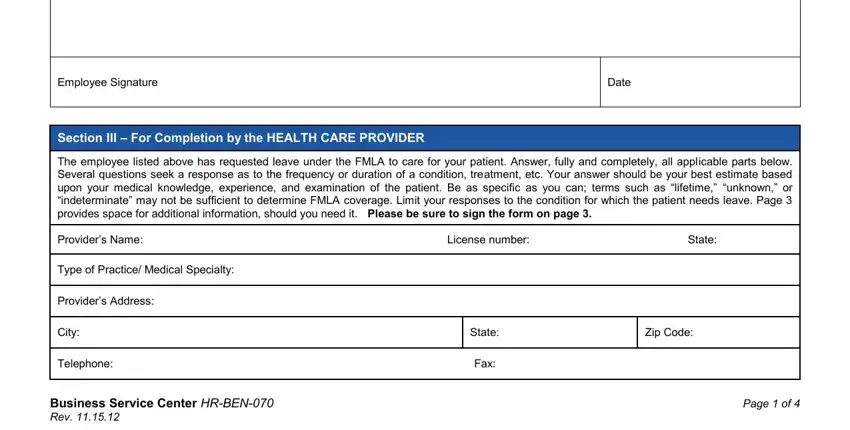
Be really mindful when filling in Telephone Fax and Providers Address, as this is the part in which most people make a few mistakes.
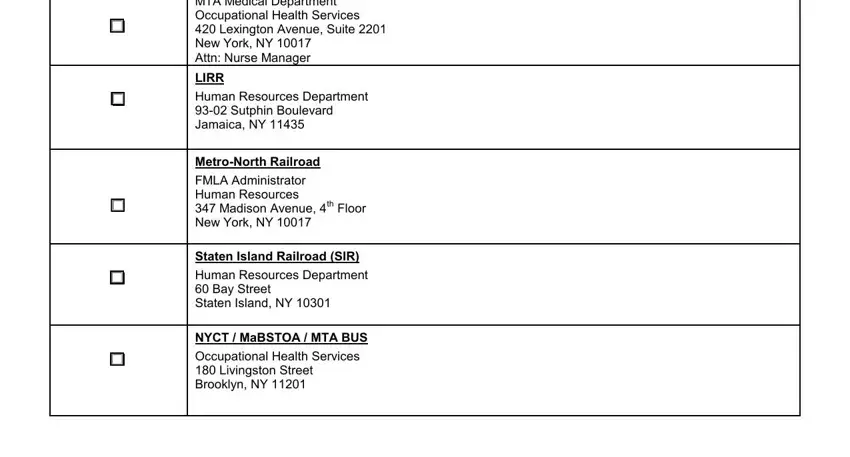
3. Completing MTA Medical Department, LIRR, Human Resources Department, MetroNorth Railroad, FMLA Administrator Human Resources, Staten Island Railroad SIR, Human Resources Department Bay, NYCT MaBSTOA MTA BUS, and Occupational Health Services is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!
Step 3: Ensure your details are right and then click "Done" to conclude the task. Sign up with FormsPal now and easily gain access to MTA, set for downloading. Each and every change you make is conveniently preserved , making it possible to customize the form later on when required. At FormsPal.com, we aim to be sure that all your information is kept secure.