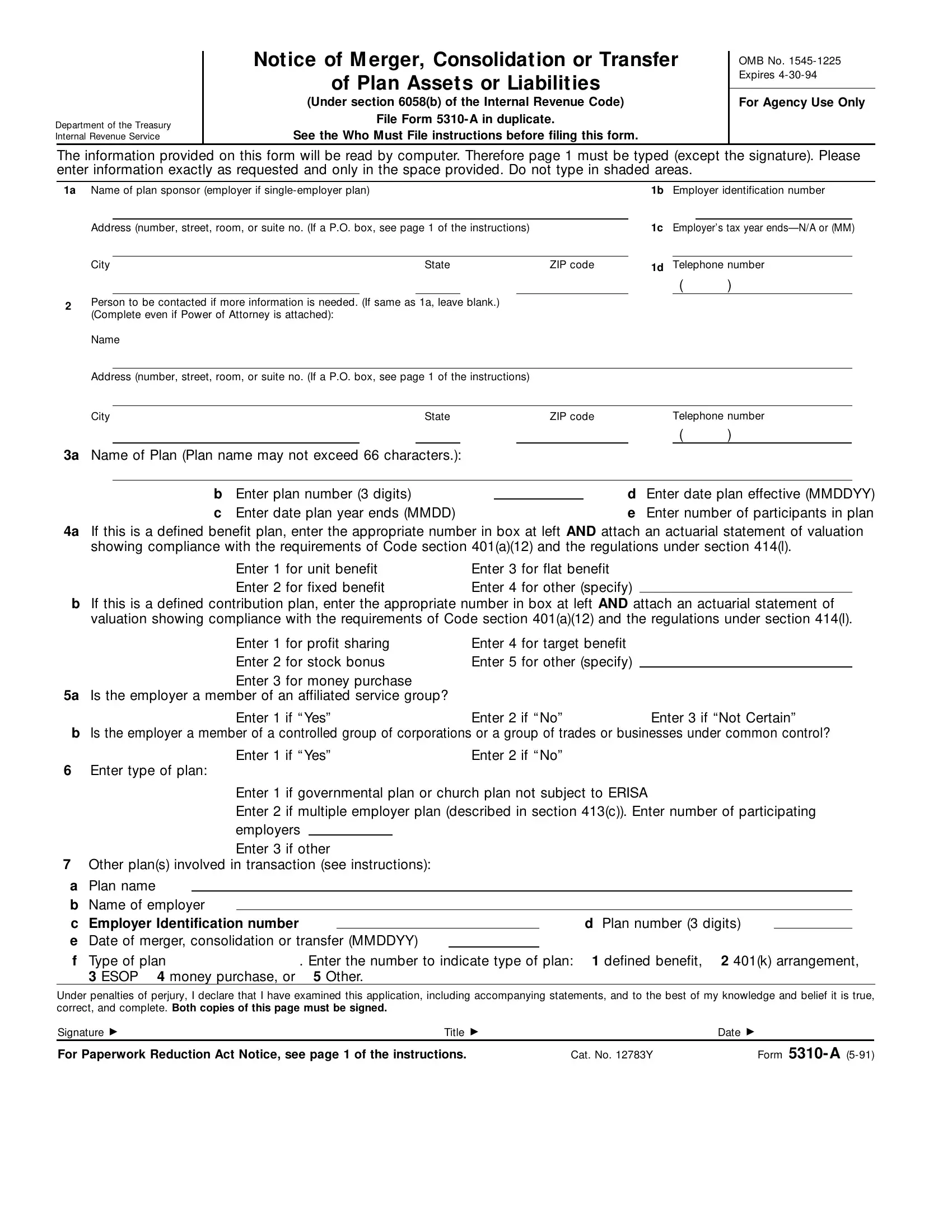
When a business undergoes big changes like mergers, consolidations, or the transferring of plan assets or liabilities, the IRS needs to be informed using Form 5310-A. This form serves a crucial role in maintaining transparency and compliance with the Internal Revenue Code, specifically under section 6058(b). It requires detailed information including the name and details of the plan sponsor, types of plans involved, and the specifics of the transaction. Preparing this form with accuracy is paramount, as it needs to be filed in duplicate and the information entered will be processed by computers. Whether the plan in question falls under a defined benefit or a defined contribution category, additional documentation like an actuarial statement of valuation might be necessary to demonstrate compliance with certain sections of the code. Other critical details include the identification of any affiliated service groups or controlled groups of corporations the employer might be a part of, and explicitly stating the number of participants in the plan. The form also demands details on other plans involved in the transaction, emphasizing its importance in cases of restructuring. By declaring the information to be true, correct, and complete under penalties of perjury, the signer acknowledges the seriousness of the form’s content. The expiration date noted, alongside the OMB number, ensures that those filing are using the most current documentation required by the Department of the Treasury and the Internal Revenue Service.
| Question | Answer |
|---|---|
| Form Name | Form 5310 A |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | Consolidation, MMDDYY, ERISA, OMB |
Department of the Treasury Internal Revenue Service
Notice of M erger, Consolidation or Transfer
of Plan Assets or Liabilities
(Under section 6058(b) of the Internal Revenue Code)
File Form 5310- A in duplicate.
See the Who Must File instructions before filing this form.
OMB No.
For Agency Use Only
The information provided on this form will be read by computer. Therefore page 1 must be typed (except the signature). Please enter information exactly as requested and only in the space provided. Do not type in shaded areas.
1a
2
Name of plan sponsor (employer if |
|
|
|
|
1b |
Employer identification number |
||||
|
|
|
|
|
|
|
|
|
||
Address (number, street, room, or suite no. (If a P.O. box, see page 1 of the instructions) |
|
1c Employer’s tax year |
||||||||
|
|
|
|
|
|
|
|
|
|
|
City |
State |
ZIP code |
1d |
Telephone number |
||||||
|
|
|
|
|
|
|
|
( |
) |
|
Person to be contacted if more information is needed. (If same as 1a, leave blank.) (Complete even if Power of Attorney is attached):
Name
Address (number, street, room, or suite no. (If a P.O. box, see page 1 of the instructions)
City |
State |
|
ZIP code |
Telephone number |
||||
|
|
|
|
|
|
|
( |
) |
3a Name of Plan (Plan name may not exceed 66 characters.):
b Enter plan number (3 digits) |
|
d Enter date plan effective (MMDDYY) |
c Enter date plan year ends (MMDD) |
|
e Enter number of participants in plan |
4a If this is a defined benefit plan, enter the appropriate number in box at left AND attach an actuarial statement of valuation showing compliance with the requirements of Code section 401(a)(12) and the regulations under section 414(l).
Enter 1 |
for unit benefit |
Enter 3 |
for flat benefit |
Enter 2 |
for fixed benefit |
Enter 4 |
for other (specify) |
bIf this is a defined contribution plan, enter the appropriate number in box at left AND attach an actuarial statement of valuation showing compliance with the requirements of Code section 401(a)(12) and the regulations under section 414(l).
Enter 1 for profit sharing |
Enter 4 for target benefit |
|
Enter 2 for stock bonus |
Enter 5 for other (specify) |
|
Enter 3 for money purchase |
|
|
5a Is the employer a member of an affiliated service group? |
|
|
Enter 1 if “ Yes” |
Enter 2 if “ No” |
Enter 3 if “Not Certain” |
bIs the employer a member of a controlled group of corporations or a group of trades or businesses under common control?
Enter 1 if “ Yes” |
Enter 2 if “ No” |
6 Enter type of plan:
Enter 1 if governmental plan or church plan not subject to ERISA
Enter 2 if multiple employer plan (described in section 413(c)). Enter number of participating
|
|
employers |
|
|
|
|
||
|
|
Enter 3 if other |
|
|
||||
7 |
Other plan(s) involved in transaction (see instructions): |
|
|
|||||
a |
Plan name |
|
|
|
|
|
|
|
b |
Name of employer |
|
|
|
|
|
|
|
c |
Employer Identification number |
|
|
d Plan number (3 digits) |
|
|||
eDate of merger, consolidation or transfer (MMDDYY)
f Type of plan |
. Enter the number to indicate type of plan: 1 defined benefit, 2 401(k) arrangement, |
3 ESOP 4 money purchase, or |
5 Other. |
Under penalties of perjury, I declare that I have examined this application, including accompanying statements, and to the best of my knowledge and belief it is true, correct, and complete. Both copies of this page must be signed.
Signature ▶ |
Title |
▶ |
Date ▶ |
For Paperwork Reduction Act Notice, see page 1 of the instructions. |
Cat. No. 12783Y |
Form 5310- A |
|
vv |
5/91 |
vv |
|
|
Department of the Treasury Internal Revenue Service
Notice of M erger, Consolidation or Transfer
of Plan Assets or Liabilities
(Under section 6058(b) of the Internal Revenue Code)
File Form 5310- A in duplicate.
See the Who Must File instructions before filing this form.
OMB No.
For Agency Use Only
The information provided on this form will be read by computer. Therefore page 1 must be typed (except the signature). Please enter information exactly as requested and only in the space provided. Do not type in shaded areas.
1a Name of plan sponsor (employer if |
1b Employer identification number |
2
3a
4a
v |
|
|
|
|
|
|
|
v |
v |
|
v |
Address (number, street, room, or suite no. (If a P.O. box, see page 1 of the instructions) |
1c Employer’s tax year |
||||||||||
v |
|
|
|
|
|
|
|
v |
|
|
|
City |
|
|
State |
|
|
ZIP code |
1d |
Telephone number |
|||
v |
|
v |
v |
|
v |
v |
|
v |
( |
) |
|
Person to be contacted if more information is needed. (If same as 1a, leave blank.) |
|
|
|
|
|||||||
(Complete even if Power of Attorney is attached): |
|
|
|
|
|
|
|
|
|
|
|
Name |
|
|
|
|
|
|
|
|
|
|
|
v |
|
|
|
|
|
|
|
|
|
|
v |
Address (number, street, room, or suite no. (If a P.O. box, see page 1 of the instructions) |
|
|
|
|
|||||||
v |
|
|
|
|
|
|
|
|
|
|
v |
City |
|
|
State |
|
|
ZIP code |
|
Telephone number |
|||
v |
|
v |
v |
|
v |
v |
|
v |
( |
) |
|
Name of Plan (Plan name may not exceed 66 characters.):
v |
|
|
|
|
|
|
|
|
v |
v |
v |
b |
Enter plan number (3 digits) |
|
|
|
d |
Enter date plan effective (MMDDYY) |
|
v |
v |
c |
Enter date plan year ends (MMDD) |
v |
|
v |
e |
Enter number of participants in plan |
|
If this is a defined benefit plan, enter the appropriate number in box at left AND attach an actuarial statement of valuation showing compliance with the requirements of Code section 401(a)(12) and the regulations under section 414(l).
v |
v |
Enter 1 for unit benefit |
Enter 3 for flat benefit |
Enter 2 for fixed benefit |
Enter 4 for other (specify) |
bIf this is a defined contribution plan, enter the appropriate number in box at left AND attach an actuarial statement of valuation showing compliance with the requirements of Code section 401(a)(12) and the regulations under section 414(l).
v
v
Enter 1 for profit sharing |
Enter 4 for target benefit |
Enter 2 for stock bonus |
Enter 5 for other (specify) |
Enter 3 for money purchase
5a Is the employer a member of an affiliated service group?
v |
v |
Enter 1 if “ Yes” |
Enter 2 if “ No” |
Enter 3 if “ Not Certain” |
bIs the employer a member of a controlled group of corporations or a group of trades or businesses under common control?
v |
v |
6Enter type of plan:
Enter 1 if “ Yes”
Enter 2 if “ No”
v |
v |
Enter 1 if governmental plan or church plan not subject to ERISA |
||
|
|
Enter 2 if multiple employer plan (described in section 413(c)). Enter number of participating |
||
|
|
employers |
|
|
Enter 3 if other
7Other plan(s) involved in transaction (see instructions):
a |
Plan name |
v |
|
|
|
|
|
|
|
|
|
|
v |
b |
Name of employer |
v |
|
|
|
|
|
|
|
|
v |
||
c |
Employer Identification number |
v |
|
|
|
v |
d Plan number (3 digits) v |
|
v |
||||
e |
Date of merger, consolidation or transfer (MMDDYY) |
v |
|
v |
|
|
|
||||||
f |
Type of plan |
v |
|
v |
. Enter the number to indicate type of plan: |
1 defined benefit, 2 401(k) arrangement, |
|||||||
|
3 ESOP 4 money purchase, or |
5 Other. |
|
|
|
|
|
|
|||||
Under penalties of perjury, I declare that I have examined this application, including accompanying statements, and to the best of my knowledge and belief it is true, correct, and complete. Both copies of this page must be signed.
Signature ▶ |
Title |
▶ |
Date ▶ |
For Paperwork Reduction Act Notice, see page 1 of the instructions. |
Cat. No. 12783Y |
Form 5310- A |
|