Every year, the IRS releases a new Form 824L to help organizations calculate their excise tax liability. The form is used to determine the tax base for certain fuels and lubricants, and helps businesses understand their tax obligations. This year, the form has been updated to include new provisions from the Tax Cuts and Jobs Act. organizations should be sure to use the latest version of the form when calculating their taxes. For more information on how to use Form 824L, visit the IRS website.
| Question | Answer |
|---|---|
| Form Name | Form 824L |
| Form Length | 11 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 2 min 45 sec |
| Other names | 824L, social history assessment example, social history template, DHS |

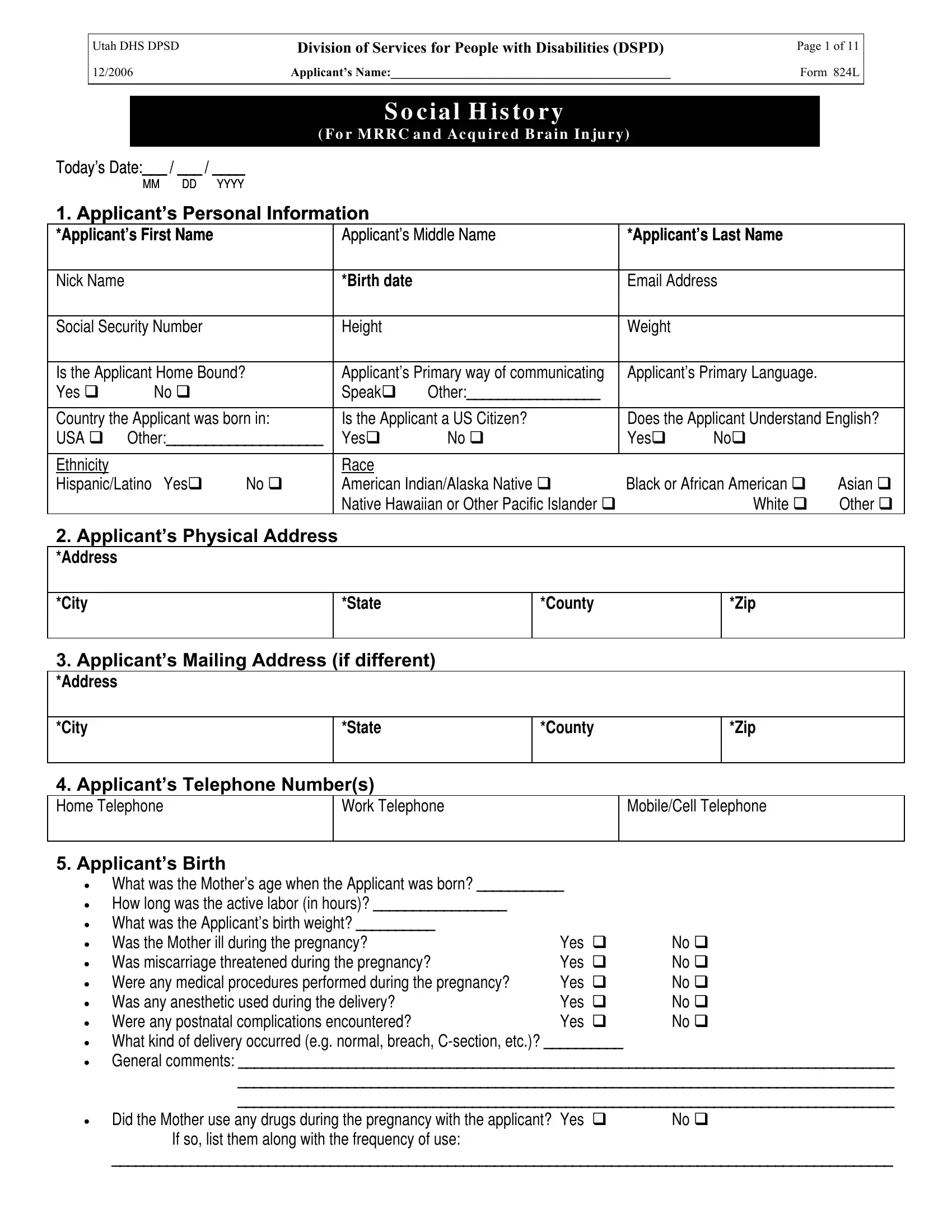
Utah DHS DPSD |
Division of Services for People with Disabilities (DSPD) |
Page 1 of 11 |
12/2006 |
Applicant’s Name:_____________________________________________ |
Form 824L |
|
|
|
S o c i a l H i s to r y
( Fo r M R R C a n d Ac q u i r e d B r a i n In ju r y)
Today’s Date:___ / ___ / ____
|
MM |
DD |
YYYY |
|
|
|
|
|
|
|
|
1. Applicant’s Personal Information |
|
|
|
|
|
|
|||||
*Applicant’s First Name |
|
|
Applicant’s Middle Name |
*Applicant’s Last Name |
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
Nick Name |
|
|
|
|
*Birth date |
|
|
Email Address |
|
||
|
|
|
|
|
|
|
|
|
|
||
Social Security Number |
|
|
Height |
|
|
Weight |
|
|
|
||
|
|
|
|
|
|
|
|||||
Is the Applicant Home Bound? |
|
Applicant’s Primary way of communicating |
Applicant’s Primary Language. |
|
|||||||
Yes |
No |
|
|
Speak |
Other:_________________ |
|
|
|
|
||
|
|
|
|
|
|
||||||
Country the Applicant was born in: |
|
Is the Applicant a US Citizen? |
Does the Applicant Understand English? |
||||||||
USA |
Other:____________________ |
|
Yes |
No |
Yes |
No |
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
Ethnicity |
|
|
|
|
Race |
|
|
|
|
|
|
Hispanic/Latino |
Yes |
No |
|
American Indian/Alaska Native |
Black or African American |
Asian |
|||||
|
|
|
|
|
Native Hawaiian or Other Pacific Islander |
|
|
White |
Other |
||
2. Applicant’s Physical Address |
|
|
|
|
|
|
|
||||
*Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
*City |
|
|
|
|
*State |
|
*County |
|
|
*Zip |
|
|
|
|
|
|
|
|
|||||
3. Applicant’s Mailing Address (if different) |
|
|
|
|
|||||||
*Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
*City |
|
|
|
|
*State |
|
*County |
|
|
*Zip |
|
|
|
|
|
|
|
|
|
||||
4. Applicant’s Telephone Number(s) |
|
|
|
|
|
|
|||||
Home Telephone |
|
|
|
Work Telephone |
Mobile/Cell Telephone |
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
5. Applicant’s Birth
•
•
•
•
•
•
•
•
•
•
•
What was the Mother’s age when the Applicant was born? ___________ |
|
|
How long was the active labor (in hours)? _________________ |
|
|
What was the Applicant’s birth weight? __________ |
|
|
Was the Mother ill during the pregnancy? |
Yes |
No |
Was miscarriage threatened during the pregnancy? |
Yes |
No |
Were any medical procedures performed during the pregnancy? |
Yes |
No |
Was any anesthetic used during the delivery? |
Yes |
No |
Were any postnatal complications encountered? |
Yes |
No |
What kind of delivery occurred (e.g. normal, breach,
General comments: ____________________________________________________________________________________
____________________________________________________________________________________
____________________________________________________________________________________
Did the Mother use any drugs during the pregnancy with the applicant? Yes |
No |
If so, list them along with the frequency of use: |
|
____________________________________________________________________________________________________

Utah DHS DPSD |
Division of Services for People with Disabilities (DSPD) |
Page 2 of 11 |
12/2006 |
Applicant’s Name:_____________________________________________ |
Form 824L |
|
|
|
6. Applicant’s Childhood Milestones
Please identify the ages when the Applicant successfully achieved the following developmental milestones
Age First Sat Up (in months) _________ |
Age First Toileted (in months) __________ |
Age First Walked (in months) __________ |
|
|
|
Age First Talked (in months) _________________
7. Applicant’s Education History
• Age Started School: _________________ |
|
|
|
• Highest Grade Completed: ___________ |
|
|
|
• |
Years Completed: __________________ |
|
|
• |
Is the Applicant leaving the Public School System? Yes |
No |
If yes, when? __________________ |
•Special School Related Achievements:_______________________________________________________________
______________________________________________________________________________________________
List Each School the Applicant Attended (please list the most recent school first).
Name of |
*Type of School |
School |
Name of |
Date |
Date |
|
In |
Comments |
School |
(Elem., Jr./ Middle |
Phone # |
School |
Started |
Ended |
Special |
|
|
|
School, High |
|
Contact |
|
|
|
Ed? |
|
|
School, College) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Y |
N |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Y |
N |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Y |
N |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Y |
N |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Y |
N |
|
|
|
|
|
|
|
|
|
|

Utah DHS DPSD |
Division of Services for People with Disabilities (DSPD) |
Page 3 of 11 |
12/2006 |
Applicant’s Name:_____________________________________________ |
Form 824L |
|
|
|
8. Applicant’s Employment History
|
Has the Applicant ever received Supported Employment through Vocational Rehab? Y |
N |
|
|
|||||||
|
If so, what year did Applicant receive Vocational Rehab services? _____________ |
|
|
|
|
||||||
+ |
|
|
|
|
|
|
|
|
|
|
|
|
(Please list the Applicant’s most recent job first) |
|
|
|
|
|
|
|
|
||
Employer |
|
Avg. Hours/Wk |
|
Most Recent |
|
Nature of Work: |
|
Start Date |
End |
|
|
|
|
|
|
|
Hourly Wage |
|
|
|
|
Date |
|
|
|
|
|
|
|
|
Paid, with benefits |
|
|
|
|
|
|
|
|
|
|
|
Paid, without benefits |
|
|
|
|
|
|
|
|
|
|
|
Volunteer/Unpaid |
|
|
|
|
Job Title/Description: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
Type of Employment (please check one): |
|
|
|
|
||||
|
|
|
|
|
|
|
|
||||
|
|
Integrated Employment – Individual (e.g. Applicant holds/held own job in the community) |
|
|
|||||||
|
|
|
|
|
|
|
|
||||
|
|
Integrated Employment – Work Crew (e.g. Applicant holds/held job in the community as part of a work crew) |
|
|
|||||||
|
|
|
|
|
|
||||||
Work Related Issues (i.e. problems with reliability, other employees, employer, etc.): |
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
||||
Level of Satisfaction with Job (please circle): |
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Employer |
|
Avg. Hours/Wk |
|
Most Recent |
|
Nature of Work: |
|
Start Date |
End |
|
|
|
|
|
|
|
Hourly Wage |
|
|
|
|
Date |
|
|
|
|
|
|
|
|
Paid, with benefits |
|
|
|
|
|
|
|
|
|
|
|
Paid, without benefits |
|
|
|
|
|
|
|
|
|
|
|
Volunteer/Unpaid |
|
|
|
|
Job Title/Description: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
Type of Employment (please check one): |
|
|
|
|
||||
|
|
|
|
|
|||||||
|
|
Integrated Employment – Individual (e.g. Applicant holds/held own job in the community) |
|
|
|||||||
|
|
Integrated Employment – Work Crew (e.g. Applicant holds/held job in the community as part of a work crew) |
|
|
|||||||
|
|
|
|
|
|
||||||
|
|
|
|
|
|
||||||
Work Related Issues (i.e. problems with reliability, other employees, employer, etc.): |
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|||||||
Level of Satisfaction with Job (please circle): |
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Employer |
|
Avg. Hours/Wk |
|
Most Recent |
|
Nature of Work: |
|
Start Date |
End |
|
|
|
|
|
|
|
Hourly Wage |
|
|
|
|
Date |
|
|
|
|
|
|
|
|
Paid, with benefits |
|
|
|
|
|
|
|
|
|
|
|
Paid, without benefits |
|
|
|
|
|
|
|
|
|
|
|
Volunteer/Unpaid |
|
|
|
|
Job Title/Description: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
Type of Employment (please check one): |
|
|
|
|
||||
|
|
|
|
|
|||||||
|
|
Integrated Employment – Individual (e.g. Applicant holds/held own job in the community) |
|
|
|||||||
|
|
|
|
|
|||||||
|
|
Integrated Employment – Work Crew (e.g. Applicant holds/held job in the community as part of a work crew) |
|
|
|||||||
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
||||||
|
|
|
|
|
|
||||||
Work Related Issues (i.e. problems with reliability, other employees, employer, etc.): |
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|||||||
Level of Satisfaction with Job (please circle): |
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
Utah DHS DPSD |
Division of Services for People with Disabilities (DSPD) |
Page 4 of 11 |
12/2006 |
Applicant’s Name:_____________________________________________ |
Form 824L |
|
|
|
9. Applicant’s Social Adjustment
• Does the Applicant have friends? Y N
•What type of person does the Applicant prefer as a friend (e.g. someone who is older, younger, or the same age, etc.)?
____________________________________________________________________________________________________
• |
Does the Applicant take part in social activities? Y |
N |
||
• |
Does the Applicant lead a lonely life? Y |
N |
|
|
• |
Does the Applicant avoid other people? |
Y |
N |
|
• |
Does the Applicant pursue the opposite sex? |
Y |
N |
|
•Additional Comments: _________________________________________________________________________________
_______________________________________________________________________________________________________
10.Applicant’s Problems (List any major health, psychological, physical, other related problems, and diagnoses that currently affect the Applicant’s life. If the applicant has a brain injury, please indicate whether the problem occurred before or after the brain injury.)
*Problem Area
*Problem Description
Who observed/
Documented the Problem?
(e.g. Mom, Dad, Doctor, Teacher,
Sister, Brother, etc.)
Date the
Problem
Was
Resolved
11. Brain Injury
If the applicant has a brain injury, please answer the following:
When (what date) did the brain injury occur? (Please try to be as precise as possible)
Describe the nature of the brain injury.
Utah DHS DPSD |
Division of Services for People with Disabilities (DSPD) |
Page 5 of 11 |
12/2006 |
Applicant’s Name:_____________________________________________ |
Form 824L |
|
|
|
12. Applicant’s Use Of Prostheses/Specialized Equipment
Does the Applicant currently use a prosthesis or any specialized equipment? If so, list each item and whether it is used or not.
*Prosthesis/Specialized |
Description |
|
*Currently Uses? |
Equipment |
|
||
|
|
|
|
|
|
Currently Uses |
Has, but doesn’t use |
|
|
|
|
|
|
Currently Uses |
Has, but doesn’t use |
|
|
|
|
|
|
Currently Uses |
Has, but doesn’t use |
|
|
|
|
13.Applicant’s Medications (please list all of the medications the Applicant is currently taking)
*Medication Name |
*Reason for Taking The |
Prescribed By |
Date Started |
Date Stopped |
|
Medication |
|
Taking the Med |
Taking the Med |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
14.Applicant’s Utilization of Medication
•What is done to help/remind the Applicant to take their medication?______________________________________________
______________________________________________________________________________________________________
15.Substance Use
Does the Applicant currently use any substances (e.g. Alcohol, tobacco, etc.)? If so, enter the following:
Type of SubstanceFrequencyComments (Daily, Weekly, Monthly)
Utah DHS DPSD |
Division of Services for People with Disabilities (DSPD) |
Page 6 of 11 |
12/2006 |
Applicant’s Name:_____________________________________________ |
Form 824L |
|
|
|
16.Applicant’s Health Treatments (List any recent visits the Applicant made to see a medical professional – including medical
*Type of Medical |
Name of |
Treated By |
Name of |
Type of Treatment |
Treatment |
Discharge/ |
Comments |
Visit (e.g. Dental, |
Medical |
What Kind of |
Facility |
|
Start Date |
Recovery |
|
Neurological, Pediatrics, |
Professional |
Medical |
|
|
or Date of |
Date |
|
Speech Therapy, Mental |
Professional? |
|
|
|
|||
|
|
|
Visit |
|
|
||
Health) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Inpatient |
|
|
|
|
|
|
|
Inpatient w/ Meds |
|
|
|
|
|
|
|
Meds only |
|
|
|
|
|
|
|
Outpatient |
|
|
|
|
|
|
|
Outpatient w/ Meds |
|
|
|
|
|
|
|
Inpatient |
|
|
|
|
|
|
|
Inpatient w/ Meds |
|
|
|
|
|
|
|
Meds only |
|
|
|
|
|
|
|
Outpatient |
|
|
|
|
|
|
|
Outpatient w/ Meds |
|
|
|
|
|
|
|
Inpatient |
|
|
|
|
|
|
|
Inpatient w/ Meds |
|
|
|
|
|
|
|
Meds only |
|
|
|
|
|
|
|
Outpatient |
|
|
|
|
|
|
|
Outpatient w/ Meds |
|
|
|
|
|
|
|
Inpatient |
|
|
|
|
|
|
|
Inpatient w/ Meds |
|
|
|
|
|
|
|
Meds only |
|
|
|
|
|
|
|
Outpatient |
|
|
|
|
|
|
|
Outpatient w/ Meds |
|
|
|
17.Applicant’s Stay In A Nursing Facility (NF) / Intermediate Care Facility for the Mentally Retarded (ICFMR)
*Is the Applicant now, or have they ever been, a resident of a nursing home or an ICFMR? If so, please enter the following:
•Admission Date ____________
•Name of the facility ___________________________
•Discharge Date ____________
18.Applicant’s Allergies
Please list all of the Applicant’s Allergies
Type of Allergy |
Comments |
|
|
|
|
|
|
|
|
|
|
19. Applicant’s Immunizations
Fill in the Immunizations the Applicant has received.
Name of Immunization |
Date Received |
Who gave the Immunization? |
|
|
|
|
|
|
|
|
|
Utah DHS DPSD |
Division of Services for People with Disabilities (DSPD) |
Page 7 of 11 |
12/2006 |
Applicant’s Name:_____________________________________________ |
Form 824L |
|
|
|
20. Applicant’s Appetite
Is the Applicant’s current appetite: Good Fair Poor
21. Applicant’s Family Relationships
Father
*Name |
|
|
|
Birth Date |
Employed? Y |
N |
|
|
|
|
|
|
|
Occupation:_________________________ |
|
|
|
|
|
|
|
||
Deceased? Y |
N |
|
|
Adopted the Applicant? |
Telephone Number |
||
Date: _________ Cause: _____________ |
Y |
N |
|
|
|||
|
|
|
|
|
|
||
Ethnicity/Race |
|
|
|
Provides Natural Supports? |
Describe his relationship with the Applicant: (e.g. |
||
|
|
|
|
Y |
N |
good, positive, confrontational, etc.) |
|
|
|
|
|
|
|
||
Does he speak English? |
Y |
N |
Lives with the Applicant? |
|
|
||
If not, what language? ________________ |
Y |
N |
|
|
|||
|
|
|
|
|
|||
Street Address (if not living with the Applicant): |
|
|
|
||||
|
|
|
|
|
|
|
|
Mother |
|
|
|
|
|
|
|
*Name |
|
|
|
Birth Date |
Employed? Y |
N |
|
|
|
|
|
|
|
Occupation:____________ |
|
|
|
|
|
|
|
||
Deceased? Y |
N |
|
|
Adopted the Applicant? |
Telephone Number |
||
Date: _________ Cause: _____________ |
Y |
N |
|
|
|||
|
|
|
|
|
|
||
Ethnicity/Race |
|
|
|
Provides Natural Supports? |
Describe her relationship with the Applicant: |
||
|
|
|
|
Y |
N |
(e.g. good, positive, confrontational, etc.) |
|
|
|
|
|
|
|
||
Does she speak English? |
Y |
N |
Lives with the Applicant? |
|
|
||
If not, what language? ________________ |
Y |
N |
|
|
|||
|
|
|
|
|
|
|
|
Street Address (if not living with the Applicant):
Stepfather (if applicable)
*Name |
Gender |
Birth Date |
|
Lives with |
|
Provides |
Adopted the |
Describe his relationship with Applicant |
|
|
|
|
Applicant? |
|
Natural |
Applicant? |
(e.g. good, positive, confrontational, etc.) |
||
|
|
|
|
|
Supports? |
|
|
|
|
|
|
|
Y |
N |
Y |
N |
Y |
N |
|
|
|
|
|
|
|
|
|
|
|
Street Address & Telephone # (if not living with the Applicant): |
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
Stepmother (if applicable) |
|
|
|
|
|
|
|
|
|
*Name |
Gender |
Birth Date |
|
Lives with |
|
Provides |
Adopted the |
Describe his relationship with Applicant |
|
|
|
|
Applicant? |
|
Natural |
Applicant? |
(e.g. good, positive, confrontational, etc.) |
||
|
|
|
|
|
Supports? |
|
|
|
|
|
|
|
Y |
N |
Y |
N |
Y |
N |
|
|
|
|
|
|
|
|
|
|
|
Street Address & Telephone # (if not living with the Applicant):
Utah DHS DPSD |
Division of Services for People with Disabilities (DSPD) |
Page 8 of 11 |
12/2006 |
Applicant’s Name:_____________________________________________ |
Form 824L |
|
|
|
Guardian (Does the Applicant have a court appointed Legal Guardian? If so, fill in the data below.)
*Name |
|
Gender |
|
Birth Date |
Lives with |
|
|
Provides |
|
|
Describe relationship with Applicant |
||||||
|
|
|
|
|
|
|
Applicant? |
|
|
Natural |
|
|
(e.g. good, positive, confrontational, etc.) |
||||
|
|
|
|
|
|
|
|
|
|
Supports? |
|
|
|
|
|
||
|
|
|
|
|
|
|
Y |
N |
|
Y |
|
N |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
*Street Address & Telephone # (if not living with the Applicant): |
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Spouse (if the Applicant is/was married) |
|
|
|
|
|
|
|
|
|
|
|
||||||
*Name |
|
Gender |
|
Birth Date |
Lives with |
|
Marital Status |
|
|
Provides |
Describe relationship with Applicant |
||||||
|
|
|
|
|
|
|
Applicant? |
|
|
(i.e. Married, |
|
|
Natural |
(e.g. good, positive, confrontational, etc.) |
|||
|
|
|
|
|
|
|
|
|
|
|
Separated, or |
|
Supports? |
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
Divorced) |
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Y |
N |
|
|
|
|
|
Y |
N |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Street Address & Telephone # (if not living with the Applicant): |
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Siblings |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
*Name |
Gender |
|
Birth |
Lives with |
Provides |
|
Address/Telephone (if not living with the |
Describe relationship |
|||||||||
|
|
|
|
Date |
Applicant? |
Natural |
|
|
|
|
Applicant) |
|
with Applicant |
||||
|
|
|
|
|
|
|
|
Supports? |
|
|
|
|
|
|
(e.g. good, positive, |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
confrontational, etc.) |
|
|
|
|
|
|
Y |
N |
Y |
N |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Y |
N |
Y |
N |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Y |
N |
Y |
N |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Y |
N |
Y |
N |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Y |
N |
Y |
N |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Y |
N |
Y |
N |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Utah DHS DPSD |
Division of Services for People with Disabilities (DSPD) |
Page 9 of 11 |
12/2006 |
Applicant’s Name:_____________________________________________ |
Form 824L |
|
|
|
22.Applicant’s Other Personal Relationships [e.g. extended family, friends, etc.] (The people entered in this area are considered to be important to the applicant and contribute in some meaningful way to their daily living experiences)
Person’s |
*What is the |
Lives with |
|
Provides |
Address/Telephone (if not living with the |
Describe relationship |
|
Name |
Relationship? |
Applicant? |
|
Natural |
Applicant) |
with Applicant |
|
|
|
|
|
Supports? |
|
(e.g. good, positive, |
|
|
|
|
|
|
|
|
confrontational, etc.) |
|
|
Y |
N |
Y |
N |
|
|
|
|
|
|
|
|
|
|
|
|
Y |
N |
Y |
N |
|
|
|
|
|
|
|
|
|
|
|
|
Y |
N |
Y |
N |
|
|
|
|
|
|
|
|
|
|
|
|
Y |
N |
Y |
N |
|
|
|
|
|
|
|
|
|
|
|
|
Y |
N |
Y |
N |
|
|
|
|
|
|
|
|
|
|
|
|
Y |
N |
Y |
N |
|
|
|
|
|
|
|
|
|
|
23. Applicant’s Professional Relationships (e.g. Doctor, Dentist, School Teacher, etc.)
Professional’s
Name
*Type of
Professional
Date
Professional
Was Last Seen
Professional’s
Telephone #
Professional’s Address
Utah DHS DPSD |
Division of Services for People with Disabilities (DSPD) |
Page 10 of 11 |
12/2006 |
Applicant’s Name:_____________________________________________ |
Form 824L |
|
|
|
24. Family Tragedies
Has the Applicant’s immediate family encountered any tragedies (e.g. automobile accidents, deaths, major illnesses, etc.)? If so, list and describe them below:
What was the Incident? |
Incident Date |
Describe the Incident |
|
|
|
|
|
|
|
|
|
|
|
|
25. Family Medical History
Does the Applicant have any family members who have notable medical issues or disabilities? If so, identify and describe the issues and/or disabilities.
Describe the Medical Issues/Disabilities
26. Agencies
Is the Applicant currently involved with any city, county, state or federal agencies? If so, enter the following:
*Name of the Agency AgencyDate the Agency Contact Person Case #Comments
Telephone Involvement
NumberStarted
Utah DHS DPSD |
Division of Services for People with Disabilities (DSPD) |
Page 11 of 11 |
12/2006 |
Applicant’s Name:_____________________________________________ |
Form 824L |
|
|
|
27. Court Orders
Is the Applicant currently affected by any court orders that impact their relationship with DSPD? If so, enter the following:
What Kind of Order is it? |
Date of the Order |
Comments |
|
|
|
|
|
|
|
|
|
28. Applicant’s Income
If the Applicant has an income, enter the following information:
Type of Income (e.g. earned, |
Amount |
With What Frequency is the |
|
Is the |
retirement, Social Security, etc.) |
|
Income Received? (e.g. weekly, |
|
Income |
|
|
monthly, annually, etc.) |
|
Stable? |
|
|
|
Y |
N |
|
|
|
|
|
|
|
|
Y |
N |
|
|
|
|
|
|
|
|
Y |
N |
|
|
|
|
|
29. Assistance
Does the Applicant receive assistance from any private or government agencies? If so, enter the following information.
Type of Assistance (e.g. Food |
Describe the Assistance |
Amount |
With What Frequency is the |
Stamps, Housing, SIC, Unemployment, |
|
|
Assistance Received? (e.g. weekly, |
Charity, etc.) |
|
|
monthly, |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
30. Insurance
If the Applicant receives insurance benefits either by himself/herself or through their family, enter the following:
Is the Insurance |
Who Owns the |
What Type of Insurance is it (e.g.. |
Insurance # |
Insurance Start Date |
Primary? |
Insurance? |
Private, Medicaid, Medicare, etc.)? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Form Completed By:_________________________________________ |
Date:____________ |
Intake Worker/Support Coordinator Signature:_____________________ |
Date:______________ |
QMRP/ABISC Signature (if applicable): __________________________ |
Date:______________ |