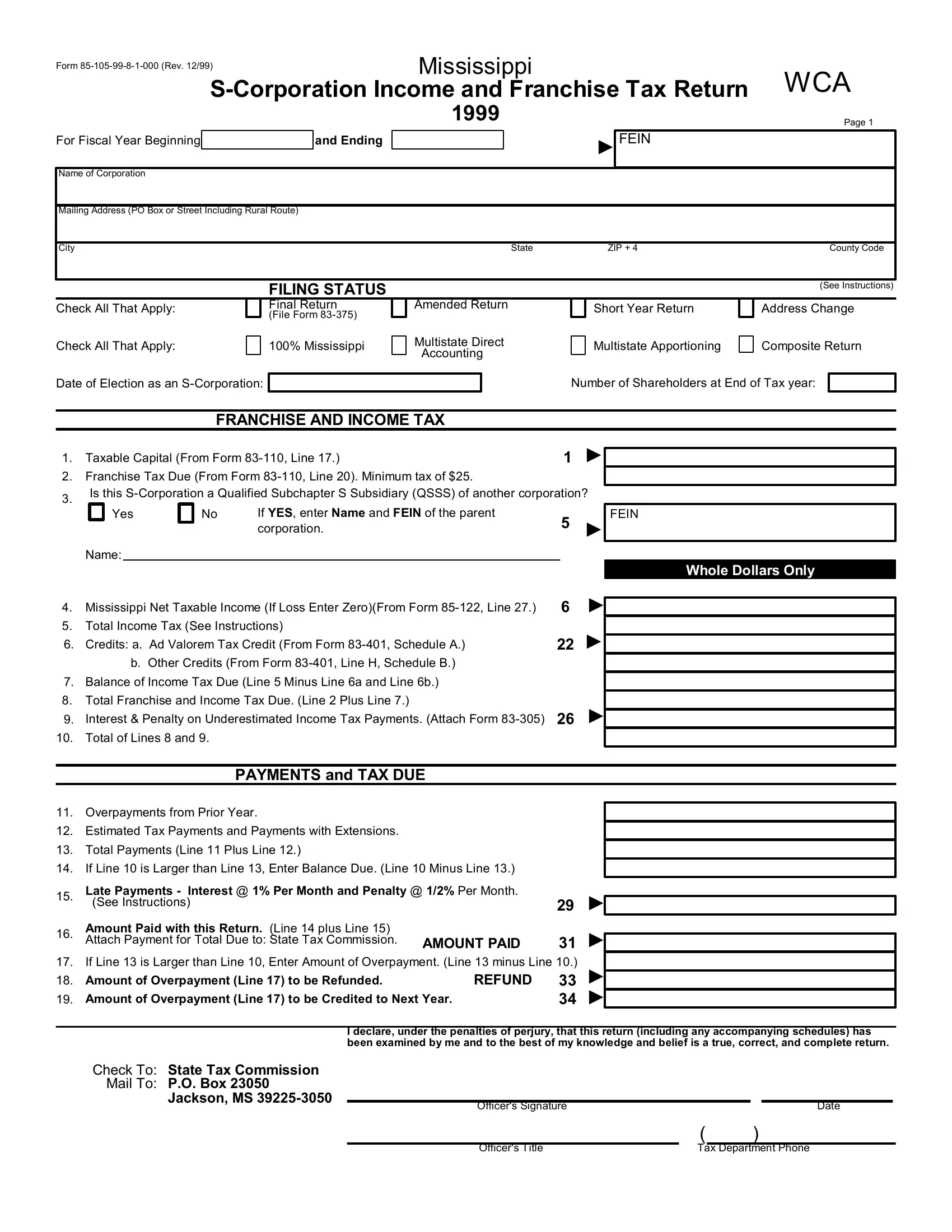
Navigating the complexities of state tax obligations can be daunting, especially for S-Corporations operating within Mississippi. The Form 85-105-99-8-1-000, a critical document revised in December 1999, serves as the Mississippi S-Corporation Income and Franchise Tax Return, catering specifically to the fiscal year starting in 1999. This form encompasses a comprehensive structure for these entities to report their income and calculate both income and franchise taxes due to the state. It addresses various filing statuses, including options for final, amended, and short year returns, while also facilitating declarations for multistate operations through direct accounting or apportioning methods. Notably, the form queries the S-Corporation's eligibility as a Qualified Subchapter S Subsidiary and prompts for details regarding the parent corporation if applicable. Beyond mere tax calculations, the form requests data on overpayments and estimated tax payments, guiding corporations through the process of rectifying any balance due or claiming refunds. Integral to ensuring accurate and compliant tax reporting, this document also entails a secondary page targeting more nuanced aspects of the S-Corporation's profile, such as business activities, product or service focus, and amendments triggered by federal tax return adjustments. Every section of this form, right down to the list of officers and the declaration of perjury, underscores the meticulous reporting standards imposed by the Mississippi State Tax Commission, making it an indispensable tool for S-Corporations navigating their fiscal responsibilities within the state.
| Question | Answer |
|---|---|
| Form Name | Form 85 105 99 8 1 000 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | 85105993 mississippi s corporation income and franchise tax return form |
