
Using PDF documents online is actually quite easy using our PDF tool. You can fill out standard history 93 here and use several other options available. To make our editor better and more convenient to use, we continuously design new features, bearing in mind feedback coming from our users. Starting is effortless! All that you should do is take the following easy steps directly below:
Step 1: Click on the "Get Form" button above. It is going to open our pdf tool so you could begin filling out your form.
Step 2: After you open the editor, you will notice the form all set to be filled out. In addition to filling out different blank fields, it's also possible to perform some other things with the file, namely putting on custom textual content, changing the initial text, adding images, signing the form, and more.
It's easy to finish the form using out detailed guide! Here is what you want to do:
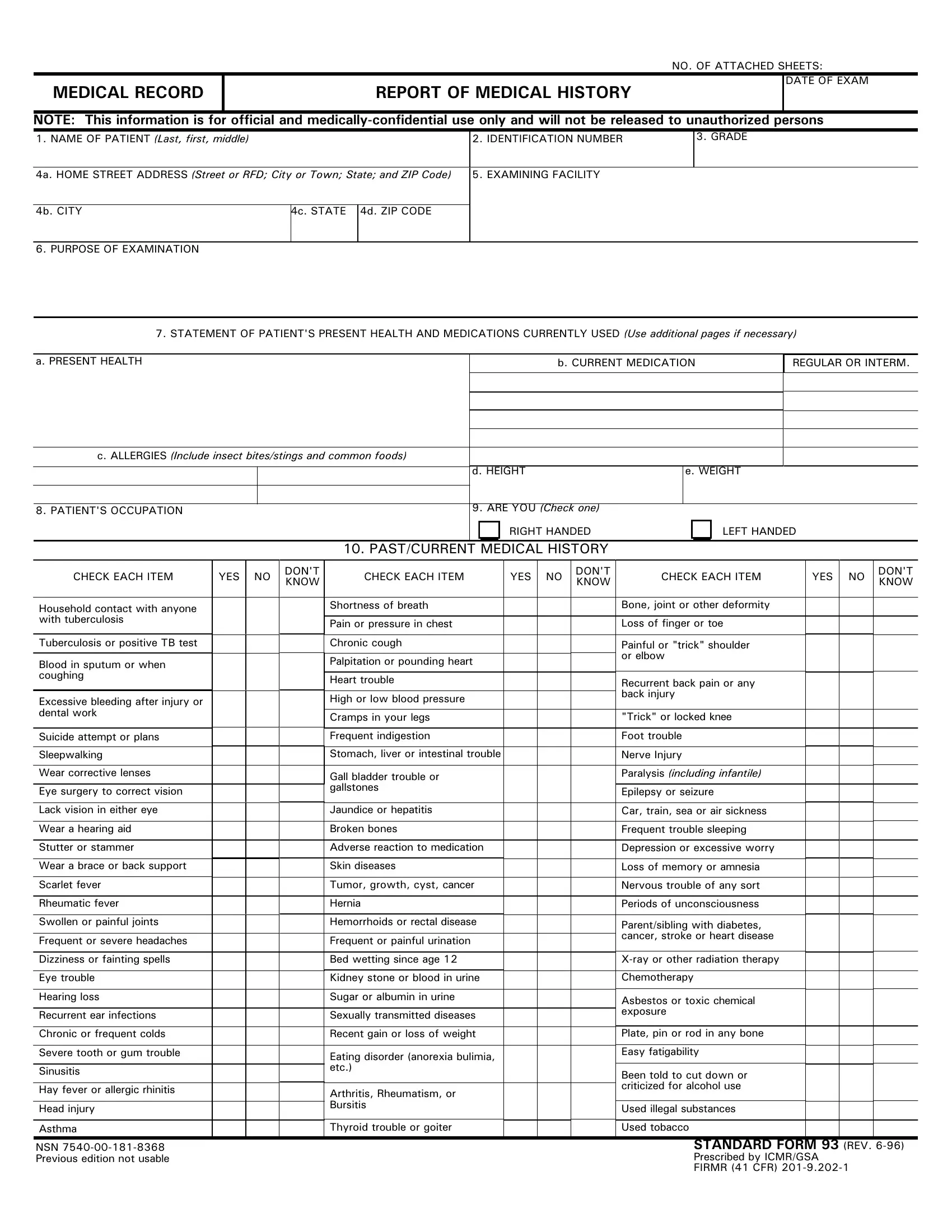
1. While completing the standard history 93, be sure to incorporate all of the necessary fields within the associated area. This will help facilitate the work, allowing your information to be processed fast and properly.
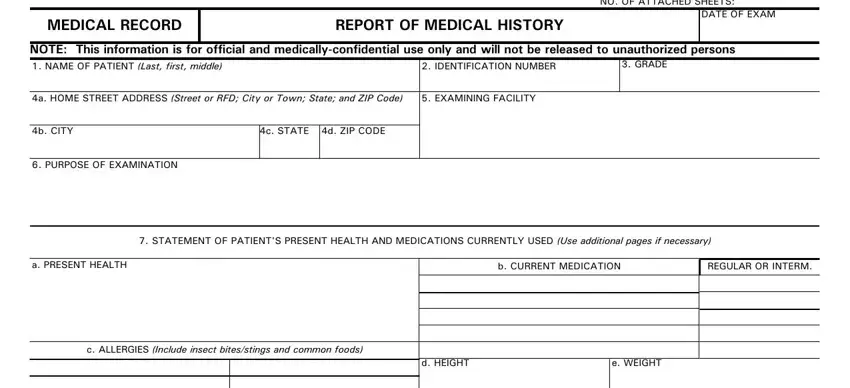
2. When the last segment is done, you're ready to add the needed details in DAA, KIADJJMEJDOA MEJDJKAHKIEI, DHJAIIBHAJD, EHFHAIIKHAEDAIJ, KAHKIEIHFIEJELAJAIJ, DHEKCD, EIFKJKHMDA KCDEC, NAIIELAAAECBJAHEKHOH AJMH, KEEAJJAFJHFI, AAFMEC, AHHHAJELAAIAI, OAIKHCAHOJHHAJLEIE, LEIEEAEJDAHAOA, AHDAHECE, and JKJJAHHIJAH allowing you to move forward to the 3rd part.
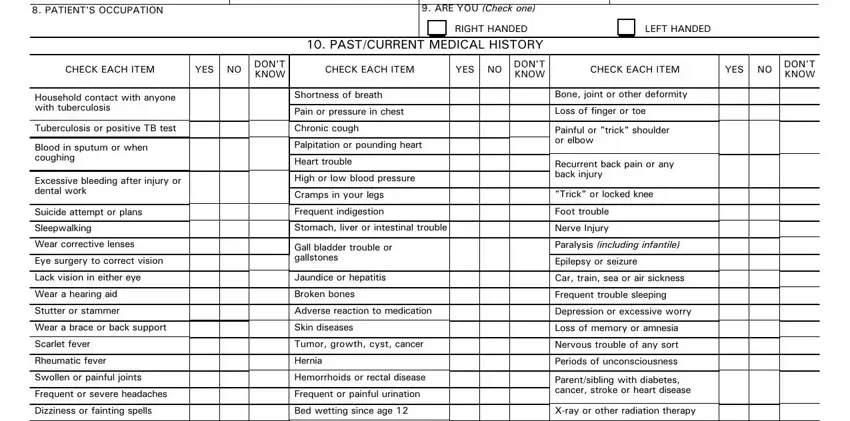
Concerning DHJAIIBHAJD and JKJJAHHIJAH, make sure you review things in this section. Those two are the most important ones in this form.
Step 3: Make certain the details are right and then click "Done" to complete the process. Obtain the standard history 93 as soon as you join for a free trial. Conveniently access the document from your personal cabinet, along with any modifications and changes being automatically saved! With FormsPal, you can fill out documents without needing to worry about personal data incidents or records getting shared. Our protected platform helps to ensure that your private details are kept safely.