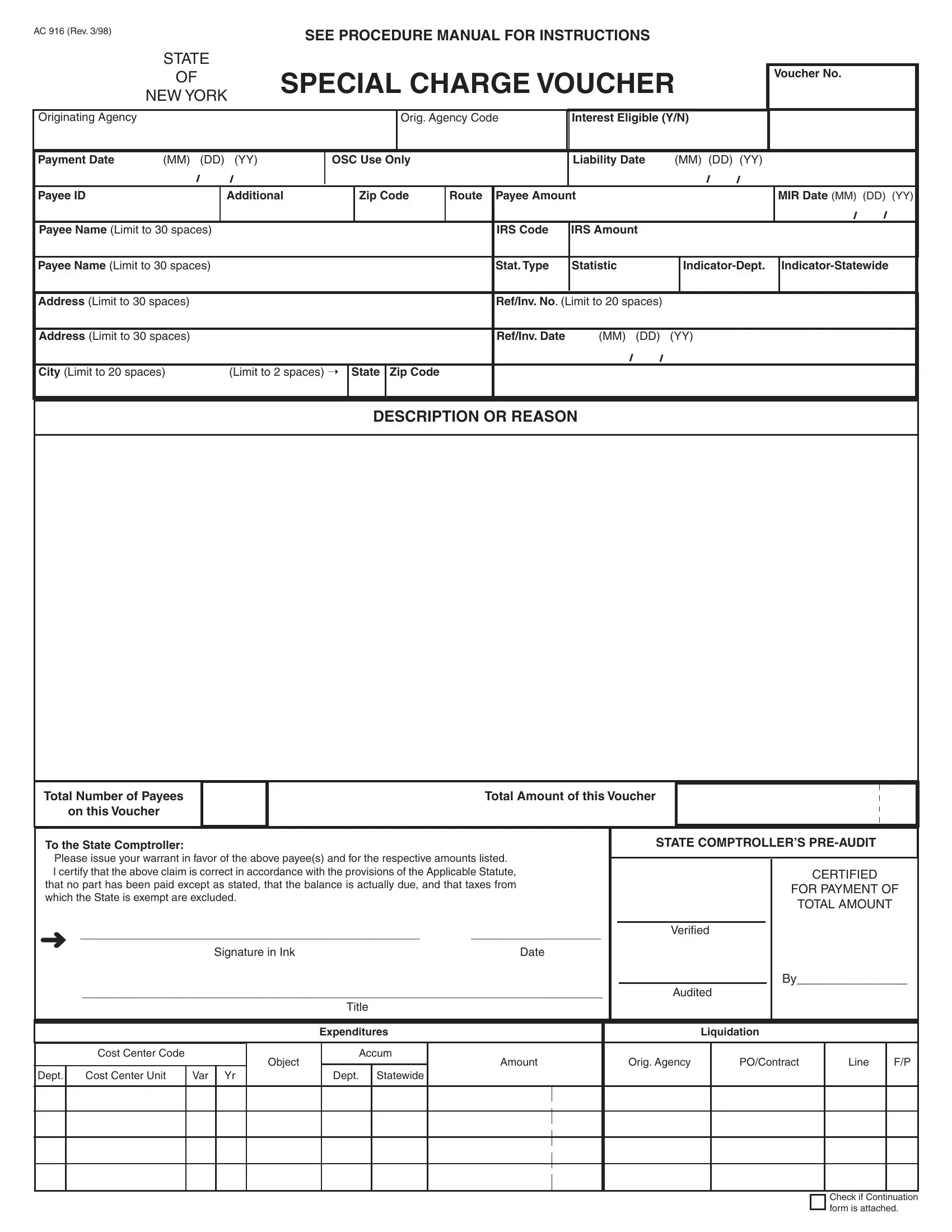
Navigating through the intricacies of government documentation can often seem overwhelming, especially when dealing with financial transactions between entities and the state. Among such pivotal documents, the AC 916 form, as per its latest revision in March 1998, stands out as a crux for processing special charge vouchers in New York. This document meticulously captures a variety of critical information, from voucher numbers to payee details and payment specifics, making it indispensable for initiating and tracking payments. It serves a dual purpose; not only does it facilitate the streamlined handling of payments by clearly outlining details such as the originating agency, the liability and payment dates, and the amount due, but it also ensures compliance with regulations through certifications and pre-audit checks. The form's layout is designed to include the payee's identification, payment reason, total amount involved, and a certification that the claim is correct, has not been previously paid, and excludes taxes from which the state is exempt. It ends with a section for the state comptroller's verification, thereby underscoring the form's importance in maintaining fiscal responsibility and integrity in transactions involving state funds.
| Question | Answer |
|---|---|
| Form Name | Form Ac 916 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | Comptroller, Accum, Payees, Orig |
AC 916 (Rev. 3/98)
SEE PROCEDURE MANUAL FOR INSTRUCTIONS
STATE
OFSPECIAL CHARGE VOUCHER
NEW YORK
Voucher No.
Originating Agency
Orig. Agency Code
Interest Eligible (Y/N)
Payment Date |
(MM) (DD) (YY) |
OSC Use Only
Liability Date |
(MM) (DD) (YY) |
Payee ID
Additional
Zip Code
Route
Payee Amount
MIR Date (MM) (DD) (YY)
Payee Name (Limit to 30 spaces)
IRS Code
IRS Amount
Payee Name (Limit to 30 spaces)
Stat. Type
Statistic
Address (Limit to 30 spaces)
Ref/Inv. No. (Limit to 20 spaces)
Address (Limit to 30 spaces)
Ref/Inv. Date |
(MM) (DD) (YY) |
City (Limit to 20 spaces) |
(Limit to 2 spaces) Ý |
State Zip Code
DESCRIPTION OR REASON
Total Number of Payees
on this Voucher
Total Amount of this Voucher
To the State Comptroller:
Please issue your warrant in favor of the above payee(s) and for the respective amounts listed.
I certify that the above claim is correct in accordance with the provisions of the Applicable Statute, that no part has been paid except as stated, that the balance is actually due, and that taxes from which the State is exempt are excluded.
Ü______________________________________________________________________________________
Signature in InkDate
______________________________________________________________________________________
Title
STATE COMPTROLLER’S
CERTIFIED
FOR PAYMENT OF
TOTAL AMOUNT
Verified
By________________
Audited
|
|
|
|
|
Expenditures |
|
Liquidation |
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cost Center Code |
|
|
Object |
Accum |
Amount |
Orig. Agency |
|
PO/Contract |
Line |
F/P |
|
|
|
|
|
|
|
|
||||||
Dept. |
Cost Center Unit |
Var |
Yr |
|
Dept. |
Statewide |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Check if Continuation form is attached.