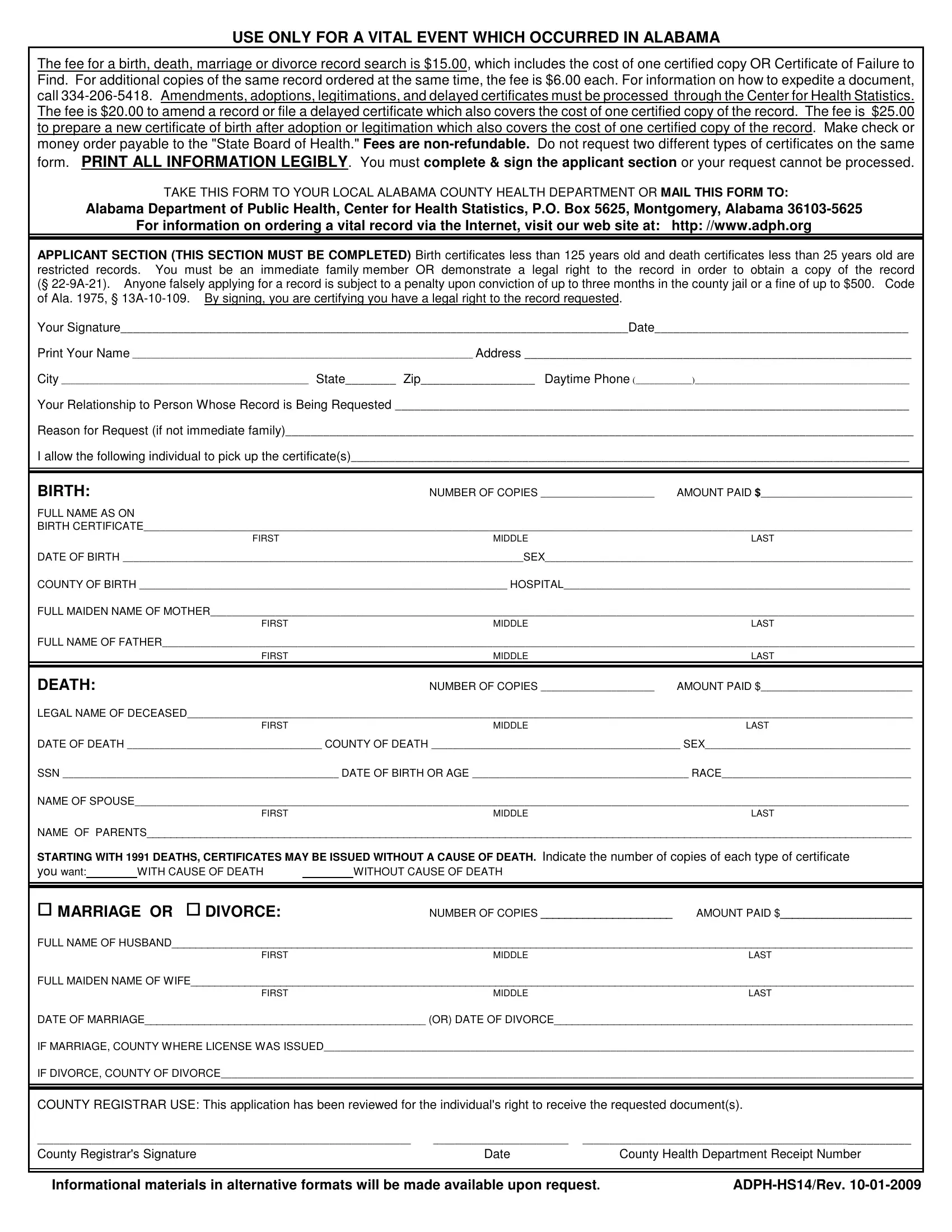
In the state of Alabama, obtaining vital records such as birth, death, marriage, or divorce certificates is facilitated through the ADPH HS14 form, a critical document governed by the Alabama Department of Public Health. This form serves as a formal request for vital event records, providing individuals with a means to access these important documents for various legal and personal reasons. The form clearly outlines the fees associated with obtaining these records, including the initial search fee of $15.00, which covers the cost of one certified copy or a Certificate of Failure to Find, and additional copies of the same record at $6.00 each. Fees for amendments, adoptions, legitimations, and delayed certificates have their own specific rates. Critical information regarding the eligibility and requirements for requesting records is detailed within the form, such as the restriction on birth certificates less than 125 years old and death certificates less than 25 years old to immediate family members or those with a legal right to the document. The significance of the ADPH HS14 form extends beyond mere record-keeping; it ensures the integrity and confidentiality of personal and familial histories, mandates the accurate completion and signing of the applicant section for processing, and sets forth penalties for fraudulent applications. By navigating the stipulations and instructions provided in the ADPH HS14 form, individuals are granted a pathway to affirming their identities, legal statuses, and genealogical connections within the jurisdiction of Alabama's health and legal frameworks.
| Question | Answer |
|---|---|
| Form Name | Form Adph Hs14 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | adph hs14, adph disinterment form, adph hs14 rev 3 2018, adph use only |
USE ONLY FOR A VITAL EVENT WHICH OCCURRED IN ALABAMA
The fee for a birth, death, marriage or divorce record search is $15.00, which includes the cost of one certified copy OR Certificate of Failure to Find. For additional copies of the same record ordered at the same time, the fee is $6.00 each. For information on how to expedite a document, call
form. PRINT ALL INFORMATION LEGIBLY. You must complete & sign the applicant section or your request cannot be processed.
TAKE THIS FORM TO YOUR LOCAL ALABAMA COUNTY HEALTH DEPARTMENT OR MAIL THIS FORM TO:
Alabama Department of Public Health, Center for Health Statistics, P.O. Box 5625, Montgomery, Alabama
For information on ordering a vital record via the Internet, visit our web site at: http: //www.adph.org
APPLICANT SECTION (THIS SECTION MUST BE COMPLETED) Birth certificates less than 125 years old and death certificates less than 25 years old are restricted records. You must be an immediate family member OR demonstrate a legal right to the record in order to obtain a copy of the record (§
Your Signature________________________________________________________________________________Date________________________________________
Print Your Name _________________________________________________________________________ Address _____________________________________________________________
City _____________________________________________________ State________ Zip__________________ Daytime Phone (____________)______________________________________________
Your Relationship to Person Whose Record is Being Requested _________________________________________________________________________________
Reason for Request (if not immediate family)___________________________________________________________________________________________________
I allow the following individual to pick up the certificate(s)________________________________________________________________________________________
BIRTH:NUMBER OF COPIES _____________________ AMOUNT PAID $____________________________
FULL NAME AS ON
BIRTH CERTIFICATE______________________________________________________________________________________________________________________________________________
FIRST |
MIDDLE |
LAST |
DATE OF BIRTH __________________________________________________________________________SEX____________________________________________________________________ |
||
COUNTY OF BIRTH ____________________________________________________________________ HOSPITAL________________________________________________________________ |
||
FULL MAIDEN NAME OF MOTHER__________________________________________________________________________________________________________________________________ |
||
FIRST |
MIDDLE |
LAST |
FULL NAME OF FATHER___________________________________________________________________________________________________________________________________________ |
||
FIRST |
MIDDLE |
LAST |
|
|
|
DEATH: |
NUMBER OF COPIES _____________________ |
AMOUNT PAID $____________________________ |
LEGAL NAME OF DECEASED______________________________________________________________________________________________________________________________________ |
||
FIRST |
MIDDLE |
LAST |
DATE OF DEATH ____________________________________ COUNTY OF DEATH ______________________________________________ SEX______________________________________
SSN ___________________________________________________ DATE OF BIRTH OR AGE ________________________________________ RACE___________________________________
NAME OF SPOUSE_______________________________________________________________________________________________________________________________________________
|
|
FIRST |
|
MIDDLE |
LAST |
NAME OF PARENTS________________________________________________________________________________________________________________________________ |
|||||
STARTING WITH 1991 DEATHS, CERTIFICATES MAY BE ISSUED WITHOUT A CAUSE OF DEATH. Indicate the number of copies of each type of certificate |
|||||
you want: |
|
WITH CAUSE OF DEATH |
|
WITHOUT CAUSE OF DEATH |
|
MARRIAGE OR DIVORCE:
NUMBER OF COPIES ______________________ |
AMOUNT PAID $______________________ |
FULL NAME OF HUSBAND____________________________________________________________________________________________________________________________
FIRSTMIDDLELAST
FULL MAIDEN NAME OF WIFE_________________________________________________________________________________________________________________________
FIRSTMIDDLELAST
DATE OF MARRIAGE_______________________________________________ (OR) DATE OF DIVORCE____________________________________________________________
IF MARRIAGE, COUNTY WHERE LICENSE WAS ISSUED_____________________________________________________________________________________________________________
IF DIVORCE, COUNTY OF DIVORCE________________________________________________________________________________________________________________________________
COUNTY REGISTRAR USE: This application has been reviewed for the individual's right to receive the requested document(s).
_____________________________________________________________________ |
_________________________ ___________________________________________________________ |
|
County Registrar's Signature |
Date |
County Health Department Receipt Number |
|
|
|
|
|
|
Informational materials in alternative formats will be made available upon request. |
||