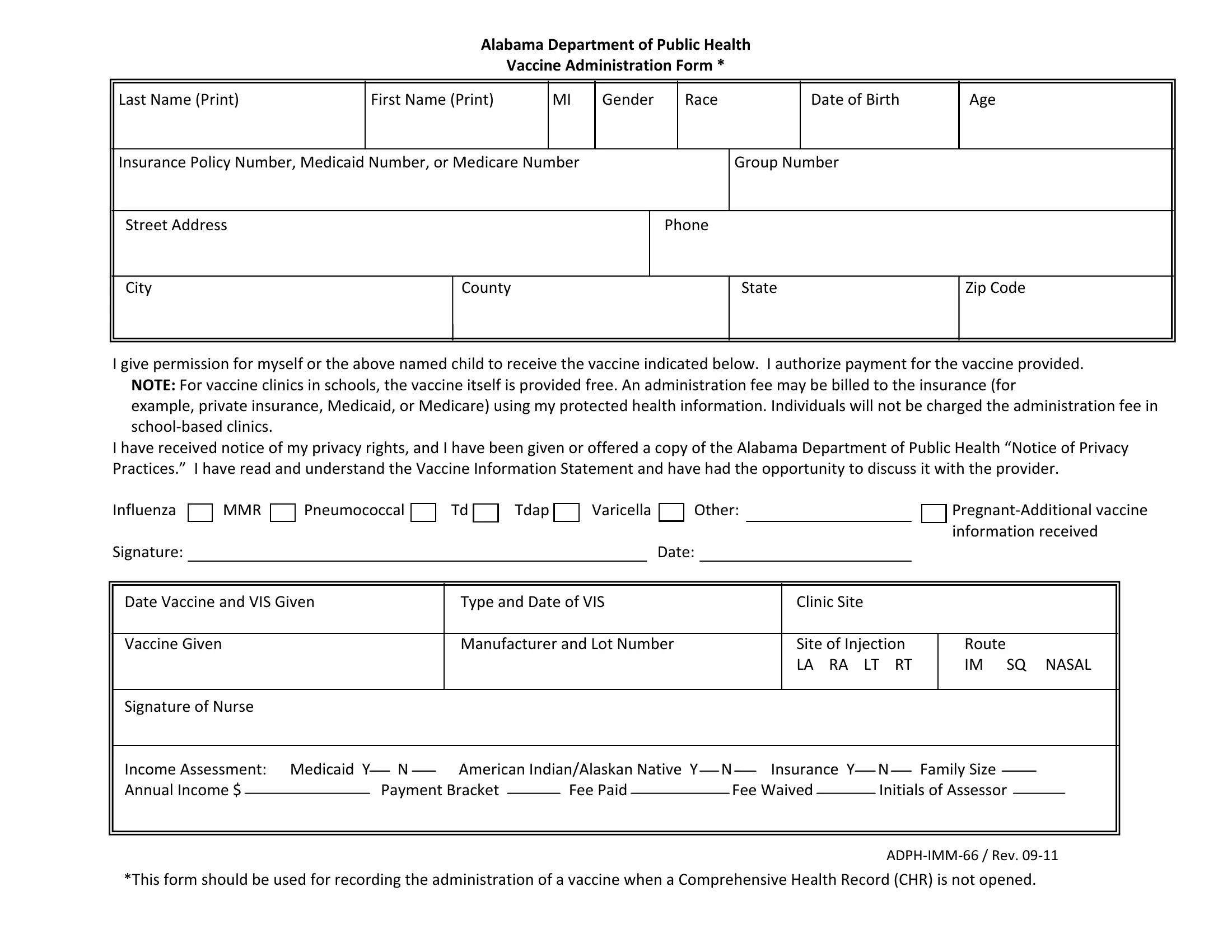
The ADPH IMM 66 form serves as a critical document within the realm of public health in Alabama, expressly designed for the meticulous recording and administration of vaccinations, particularly the flu shot. This mandatory form, as stated by the Alabama Department of Public Health, must be methodically completed to facilitate the vaccination process, ensuring patients' consent and comprehension of their privacy rights under the health department's guidelines. It requires detailed personal information, including name, contact details, and specific consent signatures, underscoring the patient or guardian's agreement to the vaccine's administration and the accompanying financial terms. Furthermore, it encapsulates vital data for healthcare providers' exclusive use, such as the vaccine's specifics—date administered, type, manufacturer, and lot number—and the patient's clinical site and method of vaccine delivery. This form also encompasses an income assessment section, which aids in determining the patient's eligibility for certain healthcare provisions, including Medicaid, thereby functioning as an indispensable tool in promoting a meticulously documented and consent-driven approach to vaccine distribution within the assurance of patient rights and privacy.
| Question | Answer |
|---|---|
| Form Name | Form Adph Imm 66 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | Bracket, RT, Medicaid, Influenza |
