

Using PDF forms online is definitely super easy with this PDF editor. You can fill in calhr 695 here and use a number of other options we provide. To maintain our editor on the leading edge of efficiency, we aim to put into operation user-driven capabilities and improvements on a regular basis. We're always looking for suggestions - join us in revolutionizing PDF editing. To begin your journey, go through these easy steps:
Step 1: Open the PDF doc inside our tool by pressing the "Get Form Button" in the top section of this webpage.
Step 2: After you start the editor, you'll see the form all set to be completed. Besides filling out different blanks, you can also do many other things with the PDF, such as writing any text, changing the initial textual content, inserting illustrations or photos, affixing your signature to the PDF, and a lot more.
In order to complete this document, ensure you type in the information you need in each and every field:
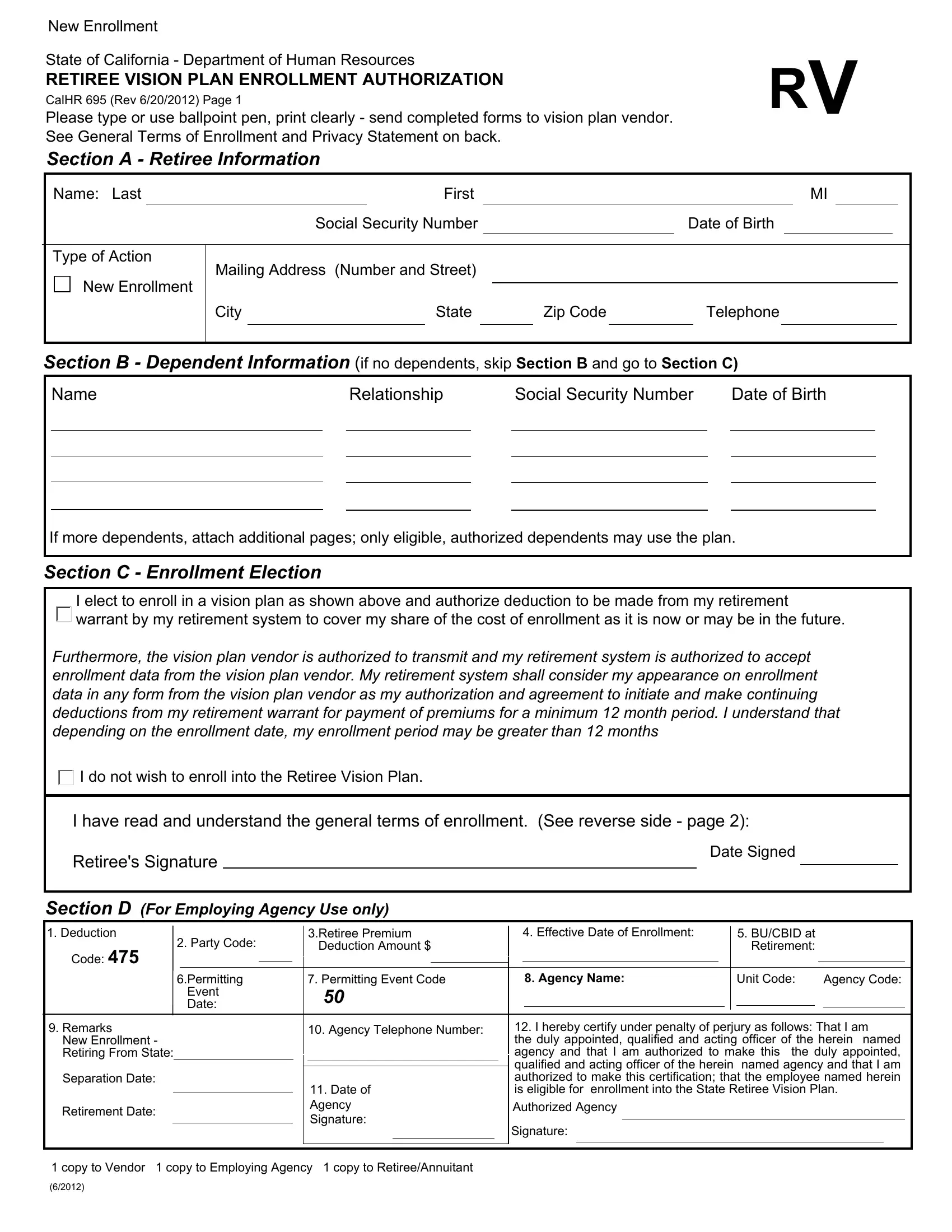
1. The calhr 695 involves certain information to be typed in. Be sure the next blank fields are filled out:
2. Once the previous array of fields is complete, you're ready insert the required details in I elect to enroll in a vision plan, Furthermore the vision plan vendor, I do not wish to enroll into the, I have read and understand the, Date Signed, Section D For Employing Agency Use, Code, Party Code, Retiree Premium Deduction Amount, Permitting Event Date, Permitting Event Code, Effective Date of Enrollment, BUCBID at Retirement, Agency Name, and Unit Code in order to go further.

Be extremely attentive while filling in Agency Name and Effective Date of Enrollment, because this is the section where many people make a few mistakes.
3. The following section is about Retirement Date, Date of Agency Signature, I hereby certify under penalty of, Signature, and copy to Vendor copy to Employing - type in each one of these fields.

Step 3: Before getting to the next stage, double-check that blank fields were filled in properly. As soon as you confirm that it is fine, press “Done." After starting afree trial account at FormsPal, you'll be able to download calhr 695 or email it promptly. The document will also be available from your personal account page with all of your changes. FormsPal provides risk-free document completion with no data record-keeping or any kind of sharing. Rest assured that your details are secure with us!