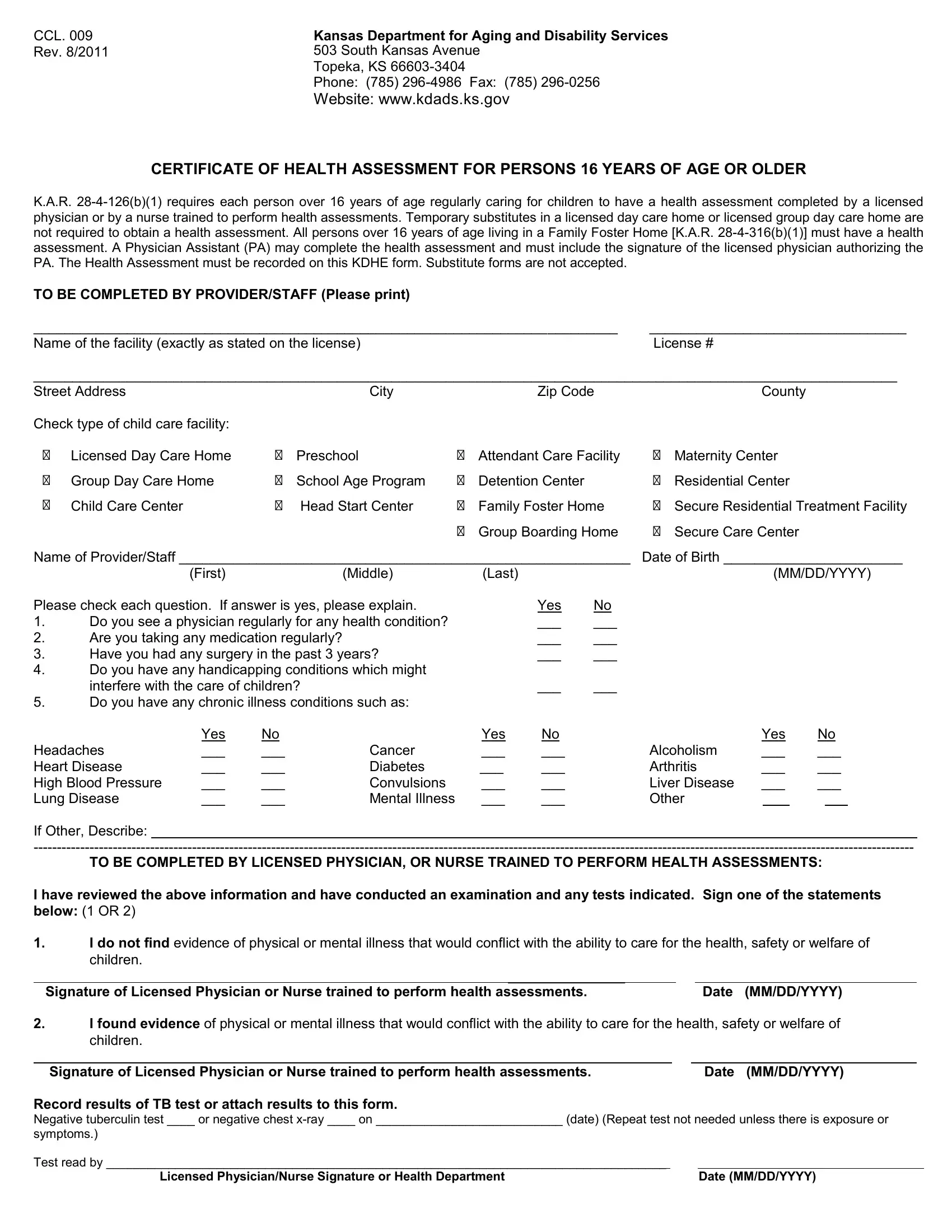
Navigating through the requirements of child and foster care in Kansas just got easier with the introduction of the CCL 009 form, a pivotal document designed to ensure the health and safety of children under care. The Kansas Department for Aging and Disability Services, anchored at 503 South Kansas Avenue in Topeka, orchestrates this regulation, mandating a thorough health assessment for individuals aged 16 and above who are regularly engaged in child care activities or residing in a Family Foster Home. Unlike temporary substitutes, these members must undergo a health assessment performed by either a licensed physician or a nurse equipped for such assessments. This measure, underscored by K.A.R. 28-4-126(b)(1) for childcare providers and K.A.R. 28-4-316(b)(1) for those in foster homes, aims to fortify the care environment's integrity. The form serves as the exclusive medium for recording these health assessments, rejecting substitute documents, and ensuring compliance through a standardized process. Its design captures essential health information, ranging from regular physician consultations, medication intake, surgical history in the past three years, to potential handicapping conditions that might affect childcare capabilities. Furthermore, it includes a detailed section for the assessing physician or nurse to conclusively document whether the individual's health status aligns with the requisites for safely caring for children, further integrated with tuberculosis testing outcomes. This comprehensive approach underscores Kansas's commitment to safeguarding child welfare within its care systems.
| Question | Answer |
|---|---|
| Form Name | Form Ccl 009 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | CCL_009_Health_ Assessment_16_ _Older department of aging form kansas how to fill out form |
CCL. 009 Rev. 8/2011
Kansas Department for Aging and Disability Services 503 South Kansas Avenue
Topeka, KS
Phone: (785)
Website: www.kdads.ks.gov
CERTIFICATE OF HEALTH ASSESSMENT FOR PERSONS 16 YEARS OF AGE OR OLDER
K.A.R.
TO BE COMPLETED BY PROVIDER/STAFF (Please print) |
|
___________________________________________________________________________ |
_________________________________ |
Name of the facility (exactly as stated on the license) |
License # |
_______________________________________________________________________________________________________________
Street Address |
|
City |
|
Zip Code |
|
County |
Check type of child care facility: |
|
|
|
|
|
|
Licensed Day Care Home |
Preschool |
Attendant Care Facility |
Maternity Center |
|||
Group Day Care Home |
School Age Program |
Detention Center |
Residential Center |
|||
Child Care Center |
Head Start Center |
Family Foster Home |
Secure Residential Treatment Facility |
|||
|
|
|
Group Boarding Home |
Secure Care Center |
||
Name of Provider/Staff __________________________________________________________ Date of Birth _______________________
|
(First) |
(Middle) |
(Last) |
|
(MM/DD/YYYY) |
Please check each question. If answer is yes, please explain. |
|
Yes |
No |
||
1. |
Do you see a physician regularly for any health condition? |
|
___ |
___ |
|
2. |
Are you taking any medication regularly? |
|
|
___ |
___ |
3. |
Have you had any surgery in the past 3 years? |
|
___ |
___ |
|
4.Do you have any handicapping conditions which might
interfere with the care of children? |
___ |
___ |
5.Do you have any chronic illness conditions such as:
|
Yes |
No |
|
Yes |
No |
|
Yes |
No |
||
Headaches |
___ |
___ |
Cancer |
___ |
___ |
Alcoholism |
___ |
___ |
||
Heart Disease |
___ |
___ |
Diabetes |
___ |
___ |
Arthritis |
___ |
___ |
||
High Blood Pressure |
___ |
___ |
Convulsions |
___ |
___ |
Liver Disease |
___ |
___ |
||
Lung Disease |
___ |
___ |
Mental Illness |
___ |
___ |
Other |
|
|
|
|
If Other, Describe:____
TO BE COMPLETED BY LICENSED PHYSICIAN, OR NURSE TRAINED TO PERFORM HEALTH ASSESSMENTS:
I have reviewed the above information and have conducted an examination and any tests indicated. Sign one of the statements below: (1 OR 2)
1.I do not find evidence of physical or mental illness that would conflict with the ability to care for the health, safety or welfare of children.
_______________ |
|
|
Signature of Licensed Physician or Nurse trained to perform health assessments. |
|
Date (MM/DD/YYYY) |
2.I found evidence of physical or mental illness that would conflict with the ability to care for the health, safety or welfare of
children. |
|
|
|
________________________ |
_ |
|
|
Signature of Licensed Physician or Nurse trained to perform health assessments. |
|
|
Date (MM/DD/YYYY) |
Record results of TB test or attach results to this form.
Negative tuberculin test ____ or negative chest
symptoms.)
Test read by _________________________________________________________________________________ |
|
Licensed Physician/Nurse Signature or Health Department |
Date (MM/DD/YYYY) |