
In case you wish to fill out Form Ccr O 24, it's not necessary to install any kind of applications - simply give a try to our online PDF editor. To keep our tool on the forefront of convenience, we strive to put into action user-driven features and improvements on a regular basis. We're at all times pleased to receive feedback - join us in reshaping the way you work with PDF documents. All it requires is just a few basic steps:
Step 1: Firstly, open the pdf editor by clicking the "Get Form Button" in the top section of this site.
Step 2: Using our online PDF editor, you can do more than merely complete blanks. Try all the features and make your documents look perfect with customized textual content put in, or optimize the original content to perfection - all backed up by the capability to incorporate your own graphics and sign it off.
As for the fields of this specific document, here is what you should consider:
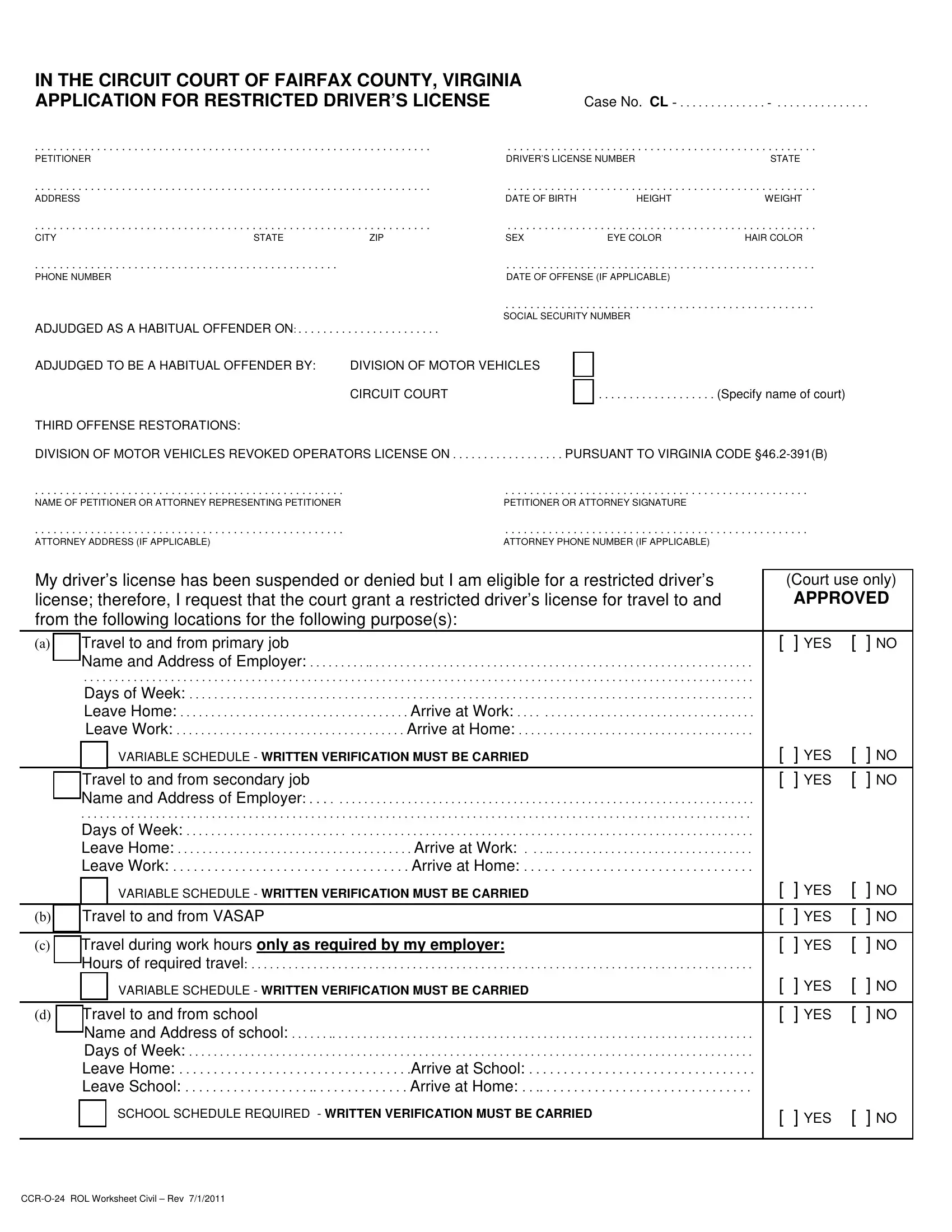
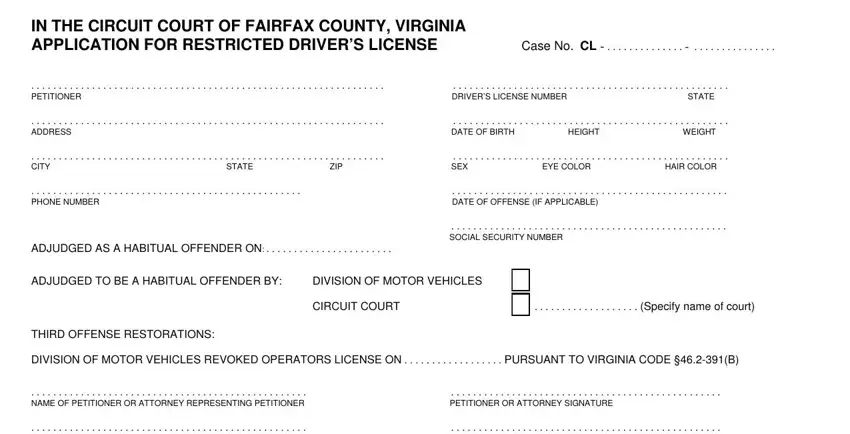
1. The Form Ccr O 24 necessitates specific details to be inserted. Ensure the next blanks are completed:
2. Given that the last section is finished, you should add the necessary details in THIRD OFFENSE RESTORATIONS, Leave Work, VARIABLE SCHEDULE WRITTEN, Travel to and from secondary job, b Travel to and from VASAP, c Travel during work hours only, d Travel to and from school, Name and Address of school, YES NO, YES NO YES NO, YES NO, YES NO, YES NO, YES NO, and YES NO so that you can move on further.
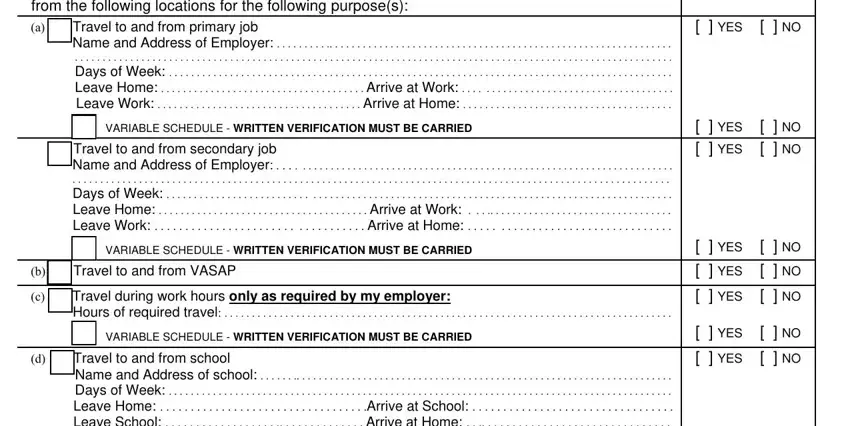
3. In this step, look at Name and Address of school, SCHOOL SCHEDULE REQUIRED WRITTEN, CCRO ROL Worksheet Civil Rev, and YES NO. Each one of these must be completed with greatest precision.

People who use this form often make errors when filling in YES NO in this section. Be sure you revise whatever you enter here.
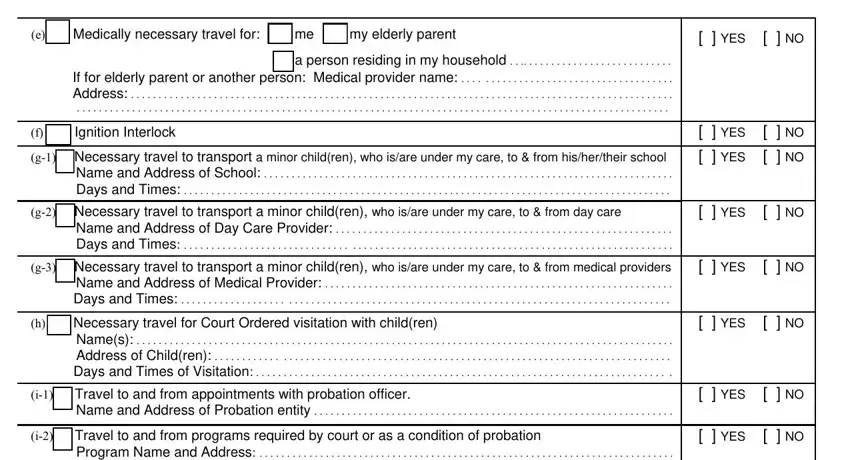
4. This paragraph comes next with the following blanks to consider: e Medically necessary travel for, If for elderly parent or another, f Ignition Interlock, g Necessary travel to transport a, g Necessary travel to transport a, g Necessary travel to transport a, h Necessary travel for Court, YES NO, YES NO, YES NO, YES NO, YES NO, YES NO, i Travel to and from, and YES NO.
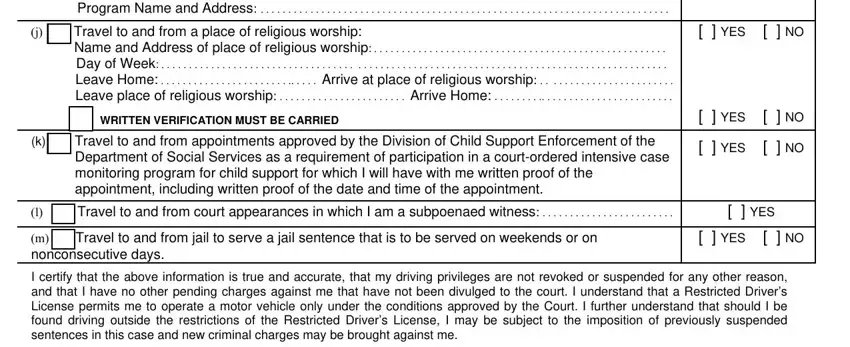
5. This very last point to conclude this form is crucial. You'll want to fill in the displayed blank fields, like i Travel to and from programs, j Travel to and from a place of, WRITTEN VERIFICATION MUST BE, k Travel to and from, Department of Social Services as a, l Travel to and from court, m Travel to and from jail to, YES NO, YES NO, YES NO, YES, YES NO, and I certify that the above, before using the document. Neglecting to do this can give you an unfinished and possibly incorrect document!
Step 3: Right after taking one more look at your filled in blanks, click "Done" and you are done and dusted! Get hold of your Form Ccr O 24 when you sign up for a 7-day free trial. Conveniently view the document from your personal account, with any edits and adjustments conveniently preserved! We don't sell or share the information that you use whenever dealing with documents at our site.