
Our PDF editor will make filling in files effortless. It is rather straightforward to update the [FORMNAME] document. Check out these particular actions in order to achieve this:
Step 1: Select the orange "Get Form Now" button on the web page.
Step 2: The form editing page is right now available. You can include text or change current details.
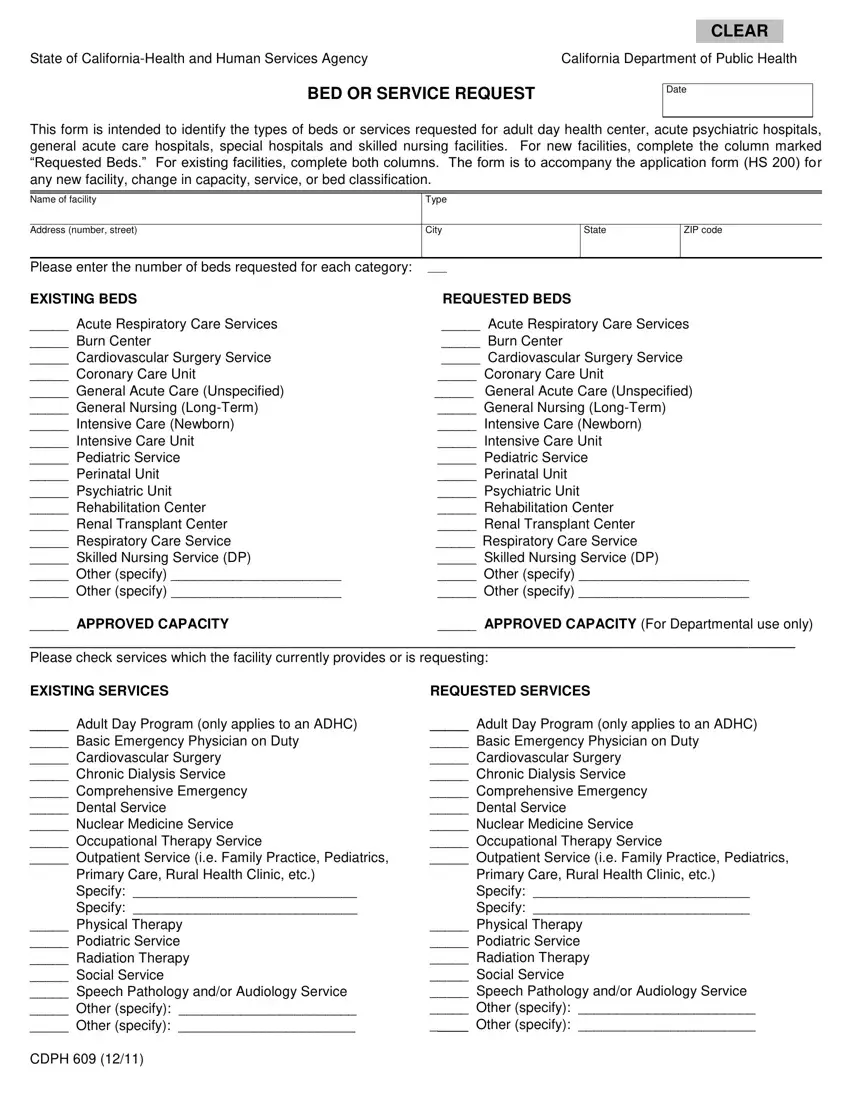
Prepare the 609 form PDF and type in the information for every single part:
Note the data in Acute Respiratory Care Services, General Acute Care Unspecified, APPROVED CAPACITY Please check, APPROVED CAPACITY For, EXISTING SERVICES, REQUESTED SERVICES, Adult Day Program only applies to, and Adult Day Program only applies to.
Note the main details in Adult Day Program only applies to, Adult Day Program only applies to, Primary Care Rural Health Clinic, Physical Therapy Podiatric, CDPH, Primary Care Rural Health Clinic, and Physical Therapy Podiatric section.
Step 3: If you are done, choose the "Done" button to upload the PDF form.
Step 4: Be sure to keep away from future complications by creating no less than two duplicates of the form.
